Francesco Amato, MD, DDS, PhD; and Giorgio Polara, DDS
ABSTRACT
The aim of this study was to investigate the performance and success rate of immediately loaded implants placed to retain fixed prostheses anchored by a novel fixed attachment system (LOCATOR F-Tx® Fixed Attachment System, Zest Dental Solutions) only removable by the clinician. Seventeen consecutive fully or partially edentulous patients were recruited to participate. Six or four implants were placed, attachments were connected, and existing dentures were immediately processed into a fixed hybrid prosthesis. No complications occurred among the 66 implants that were placed to support 17 maxillary and mandibular fixed prostheses; only one fixture failed, and all patients reported being highly satisfied. Within the limitations of this study, the use of immediately loaded implants to support prostheses that are fixed using the aforementioned attachment system appears to be a viable option for treating partially and completely edentulous patients.
Patients with edentulous arches experience numerous adverse physical and psychological effects as consequences of losing their natural teeth. Among them are difficulty speaking, eating, chewing, and otherwise ensuring proper nutrient intake; lack of self-esteem; social isolation; and dissatisfaction with their facial appearance.1,2 Although conventional removable dentures help to alleviate these problems, their instability may lead to other negative sequelae, including but not limited to stomatitis, traumatic ulcers, burning mouth syndrome, alteration of taste perception, and temporomandibular joint disorders.3,4
Additionally, the pain, discomfort, and need for unnatural lip, tongue, and cheek muscle movements to keep the prostheses in place associated with conventional removable dentures negatively interfere with patients' quality of life.1,2 Overall, in many cases the use of conventional dentures falls short of restoring patient function comfortably or satisfying patient expectations.3
Contributing to the instability of conventional dentures are residual ridge resorption and other adverse effects on the tissues supporting the dentures that occur when patients wear them.5,6 Patients who have worn conventional complete dentures for several years frequently develop severe alveolar ridge atrophy that drastically reduces the stability of the dentures.5 Ultimately, jawbone volumes are modified to the extent that patients with full-arch dentures frequently exhibit severe vertical posterior ridge resorption and horizontal anterior ridge resorption.7,8
Alternatively, the use of osseointegrated dental implants in clinical practice, which has been well documented, has become a preferred tooth-replacement option for improving the quality of life of fully edentulous patients.9,10 Osseointegration creates a firm and lasting connection between dental implants and the vital bone into which they are placed, resulting in more stable prosthetic retention and support (eg, removable bridges, overdentures) compared to conventional dentures.9,10 The use of dental implants to support overdentures increases denture stability and patient function, making the prosthesis highly stable, functionally efficient, and more comfortable.4,11 Implant-retained overdentures also help to eliminate many social, psychological, and lifestyle issues that patients may experience with traditional removable dentures.
While many patients with fully edentulous arches are candidates for implant-retained overdentures, the adverse effects of edentulism and wearing conventional removable dentures may present clinical challenges to dentists when treatment planning cases. For example, the combination of vertical posterior and horizontal anterior ridge resorptions, jawbone volume modifications, and the proximity of vital structures (eg, alveolar canal or maxillary sinus) may necessitate implant placement at different insertion axes. This could influence the correct final prosthetic outcome and mechanical force distribution.12,13 In fact, when severe atrophy is present, extreme implant angulation may be required to avoid these structures and multiple invasive regenerative procedures.14
Although placing implants at a less-than-ideal angulation helps to circumvent the issues related to implant placement in areas without adequate bone quality or quantity (eg, poor osseointegration), doing so may create other potential problems. These include a misfit between the overdenture and the implants that could lead to detrimental stress throughout the prosthesis, implant, and trabecular bone15; aggravated peri-implant bone loss and/or changes in peri-implantitis direction16; and, ultimately, implant failure. To address the challenges associated with implant angulation and non-passively fitting overdentures, several approaches have been developed to compensate for deviations from ideal positioning.
One method has been the use of cementable abutments, to include pre-angled and custom milled components, that correct for implant angulation. This abutment solution, however, requires consideration of the potential for subgingival cement, which has been associated with peri-implant diseases and subsequent implant failure.17,18 Another approach for fixed, full-arch restorations incorporates the use of straight and pre-angled screw-retained abutments. Referred to as a hybrid option, this approach has been popular because it enables clinicians to achieve the ideal angulation for connecting a prosthesis to the supporting implant; however, careful planning is required to determine the appropriate location of the screw-access hole.19 Because the exit point of screw-access holes for screw-retained components should not be on the facial aspect, the implant fixture must be positioned such that the screw-access hole emerges from either the occlusal or lingual aspect of the teeth.
These techniques can be time-consuming and in more advanced procedures, such as immediate provisionalization, may be beyond the comfort zone of some practitioners. This, combined with the risks associated with placing non-parallel implants, underscores the value of an attachment system for implant-supported prostheses that can accommodate and correct convergence/divergence between implants, eliminate the need for angled abutments, and contribute to overall survival of the final fixed prosthesis.
Research Objective
The aim of this study was to evaluate the survival rate of immediate-loaded dental implants placed in combination with a recently introduced fixed, clinician removable attachment system. (LOCATOR F-Tx® Fixed Attachment System, Zest Dental Solutions, www.zestdent.com) for the rehabilitation of edentulous patients. Using this new attachment system, the discrepancy between implant insertion axis and a patient's existing denture prosthesis would be reduced by easily modifying the angulation of the denture attachment housings given their ability to pivot on the abutment.
Material and Methods
Between March 2014 and December 2016, 15 completely edentulous patients and two partially edentulous patients who were experiencing significant discomfort due to unstable maxillary or mandibular removable dentures were enrolled in the study. The main inclusion criteria were adequate bone height (ie, >5 mm) and adequate ridge thickness (ie, >5 mm) in the edentulous area. Neither smoking nor severe systemic disorders were exclusion criteria.
Each patient underwent a complete intraoral examination and cone-beam computed tomographic (CBCT) scans. Bone quality was categorized as one of four types according to Lekholm and Zarb.20 Impressions were taken and interarch relationships recorded to mount study casts on an articulator. If possible, the existing complete removable dentures were to be utilized by processing and converting them to a fixed bridge and connecting it to the LOCATOR F-Tx abutments.
Each patient was instructed to begin systemic antibiotic prophylaxis (ie, amoxicillin 1g twice a day for 6 days) and rinse with mouthwash (ie, 0.20% chlorhexidine) 24 hours before implant placement surgery. During the surgical appointment, local anesthesia was induced using articaine 4% with adrenaline (1:100,000 Ubistesin™, 3M, 3m.com) in the vestibular and lingual areas and with adrenaline (1:50,000) in the incision line.
When the crest was wider than 7 mm and an adequate band of keratinized tissue was present, a flapless approach was preferred and undertaken. In all but one case (ie, the first), four implants (Zimmer Biomet, zimmerbiometdental.com) were inserted in the edentulous area (Table 1 and Table 2).
All osteotomies were first prepared using a piezo-surgical unit, then according to the drilling protocol suggested by the implant manufacturer, with care taken to underprepare the final diameter by at least 0.5 mm in presence of poor bone quality (Table 3). The implants were inserted using the surgical handpiece. Final seating was achieved using a calibrated torque hand ratchet to a final insertion torque, as per Table 4.
The proper abutment cuff sizes (LOCATOR F-Tx Fixed Attachment System) that had been selected during treatment planning were seated onto the implants using a dedicated LOCATOR F-Tx abutment driver included with the system (Figure 1). The abutment cuff sizes are available in different heights (ie, from 1.5 mm to 6 mm). Each abutment was then torqued to the appropriate Ncm according to the implant manufacturer's protocol.
The existing dentures were then relined. Marking paste was applied to the intaglio surface of the dentures, which were then inserted into the mouth in position over the abutments to mark the areas where the prosthesis would need to be relieved. This would allow space for the denture attachment housings to be picked up. The minimum attachment height requirement is 5.6 mm, as measured from the implant interface. The denture attachment housing is 4.1 mm in height, and this is the portion of the attachment that is processed in the prosthesis (Figure 2).
Patients were asked to close and were guided into centric occlusion, holding the position until complete setting of the resin. Occlusion was adjusted, and the patients' function with the prosthesis was assessed. The prosthesis was then removed, trimmed, adjusted, and polished (Figure 3) before being returned to the patient's mouth.
Patients were instructed to consume a liquid diet for the first 8 weeks. After that, no dietary limitations or restrictions were required.
Patients were checked once a month for the first 3 months, and then once every 6 months. At all follow-up visits, periodontal health conditions were checked for bleeding on probing and any signs of inflammation. Radiographs also were taken to evaluate bone loss. Implants were determined to be successful if they were stable, with no signs of mucositis, and if the bone levels were stable.
One month after delivery of the prosthesis, patients were asked to complete a standardized evaluation form assessing the efficacy of the implant-supported prosthesis from their perspective. Questions assessed such areas as eating, speaking ability, facial appearance, and satisfaction during daily social life (Table 5). All 17 patients responded that they were “very satisfied” with the degree of improvement in their denture's stability and chewing force.
Results
This study comprised 17 patients (ie, five males and 12 females) ranging in age from 60 to 88. Because of the investigators' initial lack of experience with the implant system, the first patient received six standard-diameter implants to minimize the risk of failure due to overloading. Thereafter, only four standard or wide-diameter implants were placed in each patient. A total of 66 implants were inserted.
The bone quality in 14 implant sites was judged to be Type 1; in 11 sites it was Type 2; in 16 sites it was Type 3; in 19 sites it was Type 4; and six sites were immediate extraction sites (Table 3). Insertion torque for the implants ranged from <30 Ncm to >90 Ncm (Table 4). For 16 patients, it was possible to use the existing dentures; for one patient, a new prosthesis was fabricated. No signs or symptoms of postoperative complications were observed.
One implant failed after 1 month; it was removed and a new fixture inserted 3 months later. After an average follow-up period of 18 months (range: 5 to 24 months) the implant success rate was 98.5%, and the prosthetic success rate was 100%.
Discussion
The LOCATOR F-Tx is a fixed attachment system that is clinician removable for rigid connection of partial (with cross-arch stabilization) and full-arch restorations on endosseous dental implants in the maxilla or mandible (Figure 4). Fixation is accomplished by a snap-in attachment that eliminates the need for subgingival cement, prosthetic screws, and screw-access channels (Figure 5). The system can be used to stabilize newly fabricated full-arch restorations (eg, all-ceramic, CAD/CAM-milled bars/bridges) or a conversion of a patient's existing full denture if the final position of the denture attachment housings within the prosthesis is acceptable. A metal frame wrapped with acrylic, PBNA, or porcelain can also be used.
Unique to the LOCATOR F-Tx Fixed Attachment System is its spherical coronal geometry, which allows the denture attachment housing to rotate in any direction and correct up to 20° from the vertical and 360° in circumference, thus allowing the attachment housing to be positioned in the ideal location for the prosthesis. This eliminates the need for angled abutments while simultaneously helping to ensure a stress-free, passive fit of the prosthesis.
Considering the clinical challenges that can result from having to place implants at different insertion axes (eg, mechanical force distribution, misfit between prosthesis and implants) that can negatively affect implant survival rates,12,13,15,16 the fact that the fixed attachment system includes a spherical coronal geometry is significant. It eliminates the need to use angled abutments or cement-retained options, thereby removing a significant known risk factor for peri-implant diseases and subsequent implant failure.17,18
Conclusion
Although many patients with fully edentulous arches are candidates for implant-supported or -retained overdentures, the adverse effects of edentulism and wearing conventional removable dentures may present clinical challenges to dentists when treatment planning cases. After having used the LOCATOR F-Tx Fixed Attachment System successfully in all applications, and based on the results of this study, the authors conclude that the adoption of this attachment system helps to resolve the issues associated with supporting fixed prostheses with implants placed at divergent insertion axes. An alternative to angled abutments, use of this fixed attachment system is time-efficient, achieves esthetically pleasing results, and is less technically complex due to the elimination of the need for cement, screw-access channels, and prosthetic screws. As with any new product, limitations and complications may occur. Therefore, clinicians must treatment plan their cases after thoroughly learning the system.
ABOUT THE AUTHORS
Francesco Amato, MD, DDS, PhD
Private Practice, Catania, Italy
Giorgio Polara, DDS
Private Practice, Modica, Italy
REFERENCES
1. Bilhan H, Geckili O, Ergin S, et al. Evaluation of satisfaction and complications in patients with existing complete dentures. J Oral Sci. 2013;55(1):29-37.
2. Hogenius S, Berggren U, Blomberg S, et al. Demographical, odontological, and psychological variables in individuals referred for osseointegrated dental implants. Community Dent Oral Epidemiol. 1992;20(4):224-228.
3. Feine JS, Maskawi K, de Grandmont P, et al. Within-subject comparisons of implant-supported mandibular prostheses: evaluation of masticatory function. J Dent Res. 1994;73(10):1646-1656.
4. Müller F, Hasse-Sander I, Hupfauf L. Studies on adaptation to complete dentures. Part I: oral and manual motor ability. J Oral Rehabil. 1995;22(7):501-507.
5. Feine JS, Carlsson GE, Awad MA, et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Montreal, Quebec, May 24-25, 2002. Int J Oral Maxillofac Implants. 2002;
17(4):601-602.
6. Pietrokovsky J, Enlow DH, Bianco HJ, Eklund S. The remodeling of the edentulous mandible. J Prosthet Dent. 1976;36(6):685-693.
7. Ueda C, Markarian RA, Sendyk CL, Lagana DC. Photoelastic analysis of stress distribution on parallel and angled implants after installation of fixed prostheses. Braz Oral Res. 2004;18(5):646-654.
8. Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg. 1988;17(4):232-236.
9. Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg. 1981;10(6):387-416.
10. Thomason JM, Lund JP, Chehade A, Feine JS. Patient satisfaction with mandibular implant overdentures and conventional dentures 6 months after delivery. Int J Prosthodont. 2003;16(5):
467-473.
11. Melilli D, Rallo A, Cassaro A. Implant overdentures: recommendations and analysis of the clinical benefits. Minerva Stomatol. 2011;60(5):251-269.
12. Misch CE. Contemporary Implant Dentistry. 2nd ed. St. Louis, MO: Mosby; 1999.
13. Barbier L, Schepers E. Adaptive bone remodeling around oral implants under axial and nonaxial loading conditions in the dog mandible. J Oral Maxillofac Implants. 1997;12(2):215-223.
14. Malo P, Nobre MA, Lopes A. Immediate rehabilitation of completely edentulous arches with a four-implant prosthesis concept in difficult conditions: an open cohort study with mean follow-up of 2 years. Int J Oral Maxillofac Implants. 2012;27(5):1177-1190.
15. Gomes EA, Assuncao WG, Tabata LF, et al. Effect of passive fit absence in the prosthesis/implant/retaining screw system: a two-dimensional finite element analysis. J Craniofac Surg. 2009;
20(6):2000-2005.
16. Arun Kumar G, Mahesh B, George D. Three dimensional finite element analysis of stress distribution around implant with straight and angled abutments in different bone qualities. J Indian Prosthodont Soc. 2013;13(4):466-472.
17. Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009;80(9):1388-1392.
18. Linkevicius T, Puisys A, Vindasiute E, et al. Does residual cement around implant-supported restorations cause peri-implant disease? A retrospective case analysis. Clin Oral Implants Res. 2013;24(11):1179-1184.
19. Wadhwani C, Piñeyro A, Avots J. An esthetic solution to the screw-retained implant restoration: introduction to the implant crown adhesive plug: clinical report. J Esthet Restor Dent. 2011;23
(3):138-143.
20. Hao Y, Zhao W, Wang Y, et al. Assessments of jaw bone density at implant sites using 3D cone-beam computed tomography. Eur Rev Med Pharmacol Sci. 2014;18(9):1398-1403.
Figures and Images

Figure 1

Figure 2

Figure 3

Figure 4
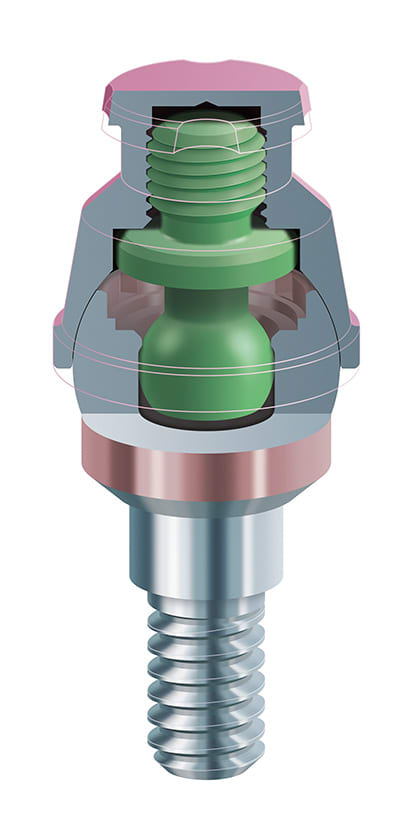
Figure 5
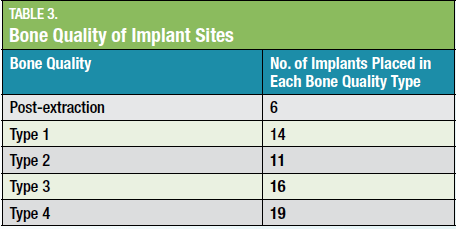
Table 1
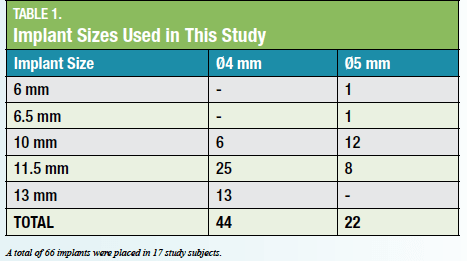
Table 2

Table 3

Table 4
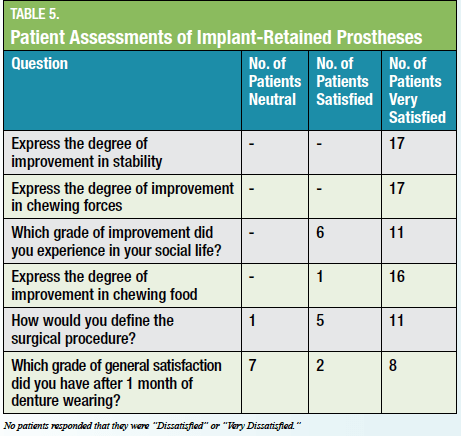
Table 5
