Pär-Olov Östman, DDS, PhD
ABSTRACT
Treatment of the edentulous patient with a fixed solution can be a challenging oral rehabilitation. Converting an existing removable denture to a fixed prosthesis using temporary cylinders and grinding holes in the denture is, in most full-arch treatments, a time-consuming procedure. Locator fixed attachments (LOCATOR F-Tx®, Zest Dental Solutions) represent a simple, predictable, and cost-effective approach to convert a patient's existing denture or install a provisional denture for immediate loading onto implants. This article reviews a study evaluating and demonstrating the ease-of-use and time-saving aspects involved in the process of using Locator fixed attachments for immediately loaded implant provisional full-arch prostheses in 13 patients. The objective was to evaluate long-term follow-up of the abutment system as well as the treatment time for fabrication of the provisional and definitive prostheses.
Individuals with completely edentulous arches are prone to several negative psychological, emotional, physical, and functional effects as direct results of their tooth loss.1,2 Although removable dentures have historically been used to replace missing teeth in an entire arch, inherent problems (eg, movement, instability, deformation) often leave patients feeling insecure, uncomfortable, and in pain due to chronic sore spots.1,2
Not surprisingly, implant-retained or -supported prostheses have gained in popularity based on their ability to stabilize the full-arch prosthesis and restore a patient to more natural function (eg, occlusal force, enhanced chewing and speaking) and esthetics (orofacial, lip, and cheek support).3 Unfortunately, traditional implant treatments often require a healing period of at least 3 months before loading the definitive overdenture or prosthesis, which may be unacceptable to many completely edentulous patients.4,5
However, research examining immediately loaded implant-supported prostheses in completely edentulous patients indicates that this approach demonstrates high success rates comparable with delayed-loaded implants.5-8 Considering the comparable success rates, among the most important advantages of immediately versus delayed-loaded implants in edentulous arches is high patient satisfaction, which has been most notable during the healing period.6 High patient satisfaction may result from the reduction in treatment time realized through immediate loading, which may explain the increasing popularity of this procedure, particularly in patients with fully edentulous arches.
From a patient perspective, there is growing interest in shortening the time frame between implant placement and installation of a functional prosthesis. The latter contributes to intraoral comfort, orofacial support, and esthetics, which can be particularly appealing and significant to patients who are professionally or socially active.3 In addition to less discomfort for patients, the fewer appointments inherent with abbreviated healing, procedures, and treatment time represents a financial and economic benefit. Likewise, from the dentist's perspective, when proper case selection and treatment planning have been completed, providing an immediately loaded prosthesis to patients with fully edentulous arches presents economic benefits. These may include less chair time for such cases and more available appointment times for other patients, each of which may help to increase profitability.
An immediately loaded implant prosthesis for the fully edentulous arch can be provided by retrofitting the patient's existing denture or installing a new provisional denture. Converting a denture to a fixed solution can be accomplished chairside by bonding temporary screw-retained cylinders into the denture base, which requires grinding holes in the denture and is often a more time-consuming process than the surgical procedure itself. It is usually performed immediately after the patient has already endured a potentially stressful surgical event.
Alternatively, a provisional prosthesis can be created in the dental laboratory after taking an implant impression during surgery, as described by many authors.9-11Although the laboratory procedure is well controlled and demonstrates several advantages over chairside provisional constructions (eg, better finishing, enhanced fit, inclusion of metal or glass fiber reinforcement, superior esthetics), extended logistics and planning are required. These provisionals involve a longer production time and tend to be more expensive. Additionally, while they typically can be delivered between 6 and 8 hours after surgery, if reinforcements are required, an extra technical working day is often necessary.
Additionally, researchers evaluating the incidence of technical complications in implants supporting a provisional bridge found that 7.4% of the restorations fractured, of which more than half occurred during the first 4 weeks.12 With an opposing implant-supported prosthesis, the fracture risk was 4.7 times higher. Bridges in the mandible, bridges without cantilevers, and those opposing natural teeth were less likely to demonstrate technical failures. The investigators studied 242 consecutive patients who were treated with 1,011 implants supporting provisional bridges during a 2- to 3-month period after surgery.
It has been this author's experience that many patients decline the option of immediate loading with a laboratory-fabricated provisional bridge due to the costs and time involved. In those cases, a chairside-made temporary construction can be a good alternative, as it provides the advantages of an immediate-loaded splinted fixed provisional that is cost-effective. However, simplifying the procedural steps involved with delivering this prosthetic option has been of interest to dentists for many years, along with availability of an easy-to-use prosthetic system that can benefit both the dentist and patient.
Technique and 3-Year Study Follow-up
The author has worked with the LOCATOR F-Tx® Fixed Attachment System (Zest Dental Solutions, zestdent.com) throughout the past 4 years. During that time, 46 patients have been treated successfully. In the first year of development, small adjustments were made to the design of the denture attachment housing and polyether ether ketone (PEEK) retentive balls. Follow-up of all the patients has shown no adverse events, and up to 4 years' follow-up has shown results comparable to traditional screw- or cement-retained full-arch rehabilitations.
A more focused study involving 13 patients was conducted to evaluate and demonstrate the ease-of-use and time-saving aspects involved in the process of using
LOCATOR F-Tx attachments for immediately loaded implant provisional full-arch prostheses. The objective was to evaluate long-term follow-up of the attachment system as well as the treatment time for fabrication of the provisional and definitive prostheses.
Material and Methods
Thirteen patients (7 female and 6 male; mean age, 57 years; range, 46-89 years) who were planned for treatment with implant-supported bridges in the edentulous maxilla and mandible participated in the study. Presurgical evaluation included clinical and radiographic examinations. Patients were selected from consecutive referrals and were considered candidates for immediate loading based on the following criteria: no general contraindications for oral surgery; 8 weeks of healing after extraction; presence of sufficient residual bone to accommodate four to six implants of at least 10 mm in length; and meeting the inclusion criteria of primary stability (ie, final torque of 30 Ncm and an implant stability quotient [ISQ] of 60 or more). All patients were thoroughly informed of the procedure and gave written consent to participate in the study. Two patients were diagnosed with diabetes mellitus type 2. Four patients were smokers.
Radiographs were taken at baseline, 3-, 6-, and 12-month follow-ups, and annually thereafter. Patients were recalled every 6 months for checkups, at which time the definitive fixed prosthesis was removed for maintenance.
Surgery
Six full-arch mandibles and seven maxillae were included. Bone quality and quantity were determined according to Lekholm and Zarb's criteria.13
All mandibular cases were treated with four implants. Three edentulous maxillae cases were treated with four implants, and four edentulous maxillae cases were treated with six implants. A total of 60 implants were installed (either T3®, Zimmer Biomet [zimmerbiometdental.com], 50 implants; or TriNex 12d Co-Axis®, Southern Implants [southernimplants.com], 10 implants).
A small fenestration was opened into the sinus to identify the anterior border of the sinus wall. After reflection of the flap, the optimal implant position was determined based on both esthetic and biomechanical considerations. Tilting the most posterior implants distally enabled placement in the most posterior position possible, reducing the need for cantilevers. Implants were placed in undersized sites to enhance primary stability.
Resonance frequency analysis (RFA) measurements were performed using an Osstell™ instrument (osstell.com). All 13 patients met the inclusion criteria of primary stability. Conversion of the patients' dentures to a fixed full-arch bridge was undertaken at the same appointment.
Temporalization
The novel spherical abutment being tested from the LOCATOR F-Tx Fixed Attachment System (Figure 1) was torqued into place on the implant using a dedicated abutment driver (Figure 2). The use of an abutment with a spherical geometry allowed the sterile denture attachment housing to pivot up to 20°, which would be significant to ensuring a stress-free, passive fit and proper alignment of the immediately loaded provisional prosthesis, as well as the definitive prosthesis.
Primary wound closure was achieved with resorbable sutures, after which the denture attachment housing was connected to the abutment and pivoted to the correct angulation alignment. The denture attachment housing is internally threaded to accept PEEK balls of various levels of retention force, in addition to a black processing ball. These balls snap into the abutment for fixation, thereby eliminating the need for extensive and time-consuming chairside procedures for retaining the prosthesis. During the procedure, the denture attachment housing (with the black ball) was snapped into the abutment and aligned to be parallel (Figure 3).
The location/position of the denture attachment housing was picked up in the denture with an index material (Figure 4). Acrylic was then removed from the denture base to accommodate the denture attachment housing, and the recesses were filled with a light-activated flowable composite (CHAIRSIDE® Attachment Processing Material, Zest Dental Solutions) (Figure 5). The denture was aligned over the denture attachment housings intraorally, with the patient closing into light occlusion, after which the flowable composite was light-cured for 3 minutes. The now-fixed denture was then removed by dislodging the black processing ball attachment that was picked up in the denture attachment housing (Figure 6). Cantilevers of 10 mm were allowed.
The black processing ball was removed and replaced with a protective polishing cap, and the denture was trimmed and polished (Figure 7). The polishing cap was removed and, depending on the number of implants, different combinations of retention balls were placed in the denture attachment housing.14 The fixed provisional prosthesis was then snapped into place intraorally, and the patient's occlusion was checked (Figure 8).
All patients were placed on mouth rinsing with chlorhexidine 2%, three times a day for 10 days, and a soft diet. After 7 to 10 days, sutures were removed, and a new combination of retention balls was selected. In three of the 13 cases, a time comparison between the LOCATOR F-Tx protocol and the classic protocol (ie, abutments and temporary cylinders) was performed.
Definitive Prosthetics
After a healing period from 8 to 10 weeks (Figure 9), an abutment-level impression was taken using the LOCATOR F-Tx impression copings and a definitive computer numerical control (CNC)-milled titanium (Ti)/acrylic or full-arch zirconia prosthesis was fabricated (Figure 10). Depending on the case, the denture attachment housing was fixated to the prosthetic framework intraorally for a completely passive fit (Ti/acrylic cases) or on the master model (zirconia), using the CHAIRSIDE attachment processing material. The manufacturer (Zest Dental Solutions) does not recommend laboratory pick-up procedures. Pick-up of housings should be done chairside if possible. High-retention balls, alone or in a combination with medium, were selected for retention of the final fixed prosthesis (Figure 11).14
Results
No implants were lost during the follow-up period. Mean final torque was 47 Ncm. Mean bone loss after 1 year of follow-up (48 out of the 60 implants) was 0.3 mm. No temporary prostheses fractured during healing time.
One temporary prosthesis dislodged during the healing period. Low-retention balls were replaced with medium-retention balls, and no further dislodgement occurred. One definitive prosthesis (four implants, 12 teeth) dislodged after final seating. Medium-retention balls were replaced with high-retention balls and, after an additional 13 months of follow-up, no dislodgement had occurred. Two denture attachment housings detached from the Ti framework during removal of the definitive prostheses at yearly checkups. Both denture attachment housings had high-retention balls attached. These findings are consistent with other evaluations in which LOCATOR F-Tx fixed attachments demonstrated few attachment-dislodgement complications.15 One of the high-retention balls fractured during removal of the fixed definitive denture. Comparatively, fracture of a screw-retained provisional prosthesis is a common finding, affecting 17% of the patients in a previous study.16.
As measured in three cases (one maxilla with six implants and two mandibles with four implants), the time required to construct a fixed temporary prosthesis from an existing denture using the LOCATOR F-Tx protocol totaled 65 minutes. Additional time saved during the remainder of treatment (ie, removing sutures, impression taking, teeth try-in, and delivery) totaled 45 minutes versus screw-retained procedures.
Discussion
As in conventional implant procedures, the outcome of treatments involving LOCATOR F-Tx fixed attachments for immediately loaded implant provisional full-arch prostheses largely depends on case selection, presurgical planning, surgical skills, and prosthetic quality. The immediate loading implant surgical procedure is comparable to conventional implant placement procedures.
However, fixation of the provisional prosthesis may, for some restorative dentists, be unfamiliar. Placement of the provisional prosthesis, which is most often performed in the presence of bleeding tissues, may require some prosthetic skills for the procedure to be efficient timewise and comfortable for the patient.
Possible drawbacks of chairside conversion of an existing prosthesis into an immediately loaded implant fixed restoration include risk of contamination of the surgical site from temporary prosthetic materials, as well as occasionally a lower esthetic outcome. These considerations must be weighed against the cost-effectiveness, time efficiency, and ease of the procedure.
Additionally, postoperative sessions for suture removal, plaque control measures, and prosthetic follow-up and modifications should be anticipated.17 The provisional prosthesis requires evaluation and, often, adaptation of occlusion and articulation.
The LOCATOR F-Tx Fixed Attachment System demonstrates advantages when modifications must be performed. Compared with a screw-retained provisional, removing LOCATOR F-Tx provisionals for corrections is less complicated and time-consuming. Although it has been suggested that early manipulation of the restoration may hamper osseointegration, removal of the provisional prosthesis on the 10th day after surgery did not jeopardize implant survival, as shown in a separate cohort study involving 71 patients.18
The LOCATOR F-Tx Fixed Attachment System also presents advantages over the classic screw-retained temporary solution in production time and risk of fractures. In the present study group, no fractures were seen. In addition, before this study, 40 additional cases were completed during the development phase of the LOCATOR F-Tx abutment system, when the product looked slightly different and the retention balls were configured differently. No fractures were seen in those 40 prestudy cases, either.
Conclusion
Within the limitations of this study, the use of a no-screw/no-cement attachment system is a viable option for immediately loaded implant-supported fixed full-arch rehabilitation. Treatment time for fabrication of provisional and definitive prostheses was reduced versus chairside traditional screw-retained techniques. Prostheses with no coping screws and no access channels to fill contributed to the lack of complications, and no fractures of the provisional or final restorations were reported. Also, the attachment system provided more pleasing esthetic results to the patients. The 3-year follow-up data show good long-term results.
ABOUT THE AUTHOR
Pär-Olov Östman, DDS, PhD
Professor, Department of Periodontology and Oral Implantology, University of Ghent, University Hospital Dental School, Ghent, Belgium
REFERENCES
1. DiMatteo A. Dentures and implants: bringing them together for a winning combination. Inside Dentistry. 2009;5(1):97-104.
2. Rossein KD. Alternative treatment plans: implant-supported mandibular dentures. Inside Dentistry. 2006;2(6):42-43.
3. Vogel RC. Implant overdentures: a new standard of care for edentulous patients—current concepts and techniques. Compend Contin Educ Dent. 2008;29(5):270-276.
4. Ho CC, Jovanovic SA. The “All-on-4” concept for implant rehabilitation of an edentulous jaw. Compend Contin Educ Dent. 2014;35(4):
255-259.
5. Lozada JL, Ardah AJ, Rungcharassaeng K, et al. Immediate functional load of mandibular implant overdentures: a surgical and prosthodontic rationale of 2 implant modalities. J Oral Implantol. 2004;30
(5):297-306.
6. De Bruyn H, Raes S, Ostman PO, Cosyn J. Immediate loading in partially and completely edentulous jaws: a review of the literature with clinical guidelines. Periodontol 2000. 2014;66(1):153-187.
7. Chiapasco M, Gatti C. Implant-retained mandibular overdentures with immediate loading: a 3- to 8-year prospective study on 328 implants. Clin Implant Dent Relat Res. 2003;5(1):29-38.
8. Tealdo T, Menini M, Bevilacqua M, et al. Immediate versus delayed loading of dental implants in edentulous patients' maxillae: a 6-year prospective study. Int J Prosthodont. 2014;27(3):207-214.
9. Aalam AA, Nowzari H, Krivitsky A. Functional restoration of implants on the day of surgical placement in the fully edentulous mandible: a case series. Clin Implant Dent Relat Res. 2005;7
(1):10-16.
10. Östman PO. Immediate/early loading of dental implants. Clinical documentation and presentation of a treatment concept. Periodontol 2000. 2008;47:90-112.
11. De Bruyn H, Van de Velde T, Collaert B. Immediate functional loading of TiOblast dental implants in full-arch edentulous mandibles: a 3-year prospective study. Clin Oral Implants Res. 2008;
ww19(7):717-723.
12. Suarez-Feito JM, Sicilia A, Angulo J, et al. Clinical performance of provisional screw-retained metal-free acrylic restorations in an immediate loading implant protocol: a 242 consecutive patients' report. Clin Oral Implants Res. 2010;21:1360-1369.
13. Lekholm U, Zarb GA. Patient selection and preparation. In: Brånemark PI, Zarb GA, Albrektsson T, eds. Tissue-integrated Prostheses: Osseointegration in Clinical Dentistry. Chicago, IL: Quintessence; 1985:199-209.
14. ELsyad MA, Agha NN, Habib AA. Retention and stability of implant-retained mandibular overdentures using different types of resilient attachments: an in vitro study. Int J Oral Maxillofac Implants. 2016;31(5):1040-1048.
15. Cakarer S, Can T, Yaltirik M, Keskin C. Complications associated with the ball, bar and locator attachments for implant-supported overdentures. Med Oral Patol Oral Cir Bucal. 2011;16
(7):e953-e959.
16. Cercadillo-Ibarguren I, Sánchez-Torres A, Figueiredo R, Valmaseda-Castellón E. Early complications of immediate loading in edentulous full-arch restorations: a retrospective analysis of 88 cases. Int J Oral Maxillofac Implants. 2017;32(5):1116–1122.
17. Kappel S, Giannakopoulos NN, Eberhard L, et al. Immediate loading of dental implants in rdentulous mandibles by use of Locator® attachments or Dolder® bars: two-year results from a prospective randomized clinical study. Clin Implant Dent Relat Res. 2016;18
(4):752-761.
18. Borges AF, Dias Pereira LA, Thome G, et al. Prostheses removal for suture removal after immediate load: success of implants. Clin Implant Dent Relat Res. 2010;12(3):244-248.
Figures and Images
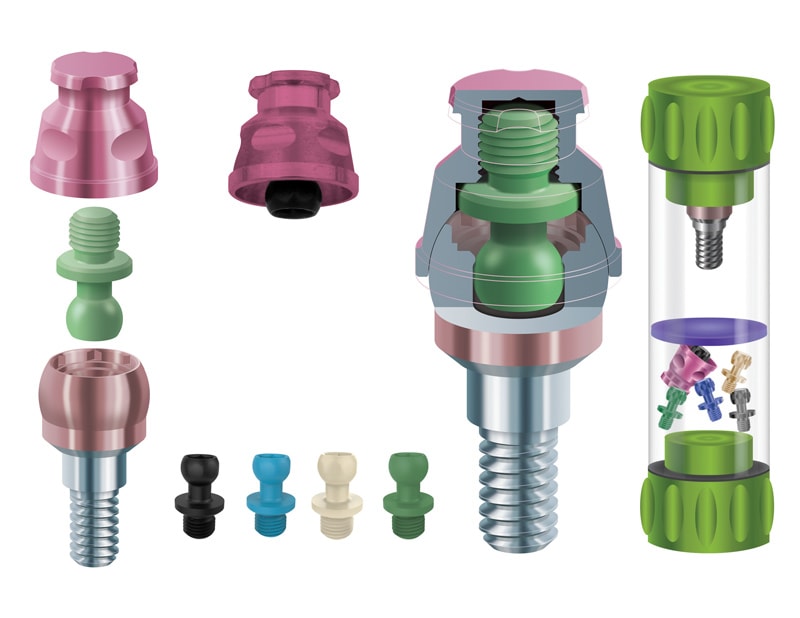
Figure 1

Figure 2
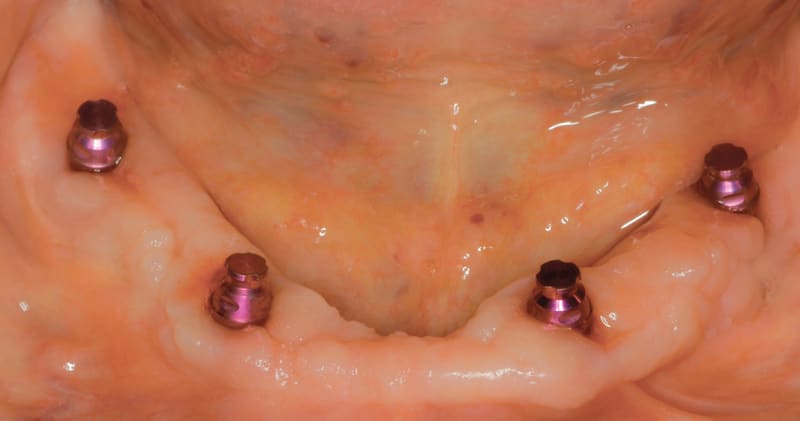
Figure 3

Figure 4

Figure 5

Figure 6

Figure 7

Figure 8
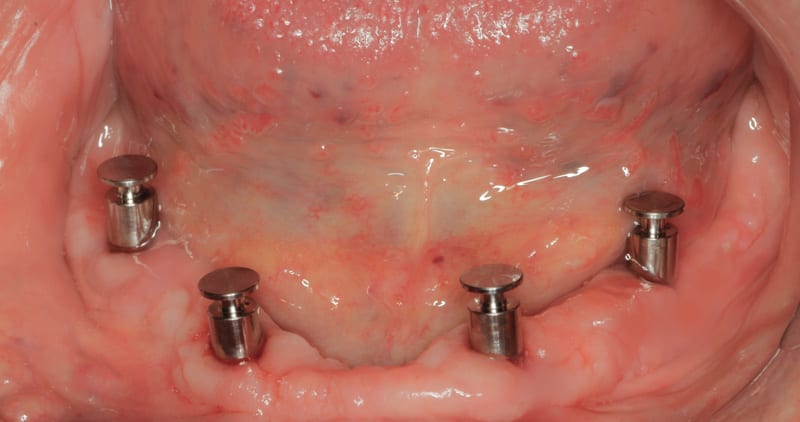
Figure 9

Figure 10

Figure 11
