SameDay Dental Implants is a team of specialist oral and maxillofacial surgeons, prosthodontists, and master dental technicians available all under one roof. With the latest computed tomography scans and 3-dimensional technology, patients in the Middle East have access to effective and painless "same day dental implant" treatment on their doorstep without having to travel to Europe or the United States. Together the team presented the following guidelines based on their extensive clinical experience for less invasive, accelerated therapy to achieve success in full-mouth rehabilitation.
Immediately Loaded Fixed Prosthesis
An immediately loaded fixed prosthesis for immediate function delivered on the same day as implant placement implies an economy and time benefit, which is especially paramount for patients with busy professional or social lives. A fixed prosthesis affords the patient comfort and confidence of function similar to real teeth.
Minimally Invasive Surgery
The concept of minimal grafting and tabling is in line with the late Professor P.I. Brånemark's philosophy of using less surgery to treat more patients. The result is less patient morbidity while potentially allowing an immediate loading protocol. Tabling, which usually is performed to satisfy prosthetic space requirements but depletes available bone, reduces anterior-posterior (A-P) spread, and converts a dental defect to a dentoalveolar defect,1 is avoided through the use of appropriate prosthetic materials. Tabling should be performed only for esthetic reasons to hide the transition line between the pink of the prosthesis and the patient's gingiva in cases of a high smile line.
Optimal Primary Stability
The implant mechanical stability at the time of surgery, known as primary stability, is the most crucial factor to enable immediate loading.2 Primary stability can be optimized by using tapered implants, by performing an underprepared osteotomy, and through osseodensification (Versah, versah.com). The Dubai SameDay team considers a minimum primary stability of 45 Ncm necessary for immediate loading.
External Connection
Benefits of the modern external hex connection with increased precision and decreased tolerance levels include: 12°, 24°, and 36° subcrestal angle correction options; a <2-μm microgap at the abutment/implant interface; and less strain on the implant and prosthetic screw.
Screw Retention
Without exception, all cases should be screw-retained and not cemented. This is made possible through the use of external hexed Co-Axis® implants (Southern Implants, southernimplants.com) with 12°, 24°, and 36° subcrestal angle correction (Figure 1). Screw retention enables retrievability for prosthetic maintenance. Additionally, there is no cement to deal with in the immediate loading environment, and there is no chance for cement-induced peri-implantitis.
Maximum A-P Spread
Biomechanically, in the "All-on-X" concept (with "X" varying from 4 to 6), the A-P spread is more important than the number of implants used. The Dubai SameDay team aims for optimal implant distribution using available native bone in the All-on-X concept. Angled/tilted implant placement can significantly increase A-P spread and decrease the length of the cantilever, which can be up to twice the length of the A-P spread in the mandible and up to 1.5 times the A-P spread in the maxilla.
Cross-Arch Stabilization With Final Prosthesis
Rigid cross-arch stabilization is necessary to splint the implants and resist micromotion. Cross-arch stabilization will also splint and protect any implant with suboptimal primary stability (<45 Ncm) as long as it is not a terminal/distal implant and the sum of the insertion torques is ≥120 Ncm to permit immediate loading.
Straight Multi-Unit Abutments
Placement of multi-unit abutments at the time of surgery (one abutment/one-time concept)3 is preferable in most multiple-implant cases unless inadequate prosthetic space dictates that the prosthesis connects directly at implant level. Furthermore, with subcrestal angle correction using 12°, 24°, and 36° Co-Axis implants, straight/0° multi-unit abutments can be used in place of cumbersome, prosthetic space-consuming 17° and 30° angled abutments (Figure 2). Multi-unit abutments result in less bone loss and increased comfort for the patient during connection/disconnection of the prosthesis.4
Site-Specific Implants
The use of site-specific implants (angled, wide, narrow) is in line with the concept of avoiding extensive bone grafting procedures. Implants are placed into available cortical bone fixation areas to allow for immediate loading. Site selection for immediate loading is completely different than site selection for delayed loading, because abundant but low-quality bone, which might be suitable for delayed loading, is not appropriate for immediate loading, as it cannot establish the required primary stability.
Site selection for site-specific implants for immediate loading is based on two principles: the presence of cortical bone, and angled/tilted implant placement to increase A-P spread and decrease cantilevers.1 Site selection for best available cortical bone for site-specific implants for immediate loading includes the following areas: anterior maxilla, piriform rim/mesial sinus wall, nasal crest/vomer, extraction sockets/lamina dura (immediate molar replacement), anterior and posterior to the sinus (tilted implants), pterygoids, and anterior mandible.
Cleansable and Maintainable Prosthesis
Prosthesis design must be user friendly, allowing access for the patient to facilitate home oral hygiene. Access for easy cleaning with needle threaders and floss is essential. Pontic design must be convex and not saddle shaped. Flange designs must be avoided.
The Presenters
Costa Nicolopoulos, BDS
SameDay Dental Implants
Petros Yuvanoglu, DMD
SameDay Dental Implants
Safa Tahmasebi, DDS, MS
SameDay Dental Implants
References
1. Jensen OT. Complete arch site classification for all-on-4 immediate function. J Prosthet Dent. 2014;112(4):741-751.
2. Gallucci GO, Benic GI, Eckert SE, et al. Consensus statements and clinical recommendations for implant loading protocols. Int J Oral Maxillofac Implants. 2014;29(suppl):287-290.
3. Degidi M, Nardi D, Piattelli A. One abutment at one time: non-removal of an immediate abutment and its effect on bone healing around subcrestal tapered implants. Clin Oral Implants Res. 2011;22(11):1303-1307.
4. Göthberg C, André U, Gröndahl K, et al. Bone response and soft tissue changes around implants with/without abutments supporting fixed partial dentures: results from a 3-year, prospective, randomized, controlled study. Clin Implant Dent Relat Res. 2016;18(2):309-322.
Figures and Images

Figure 1
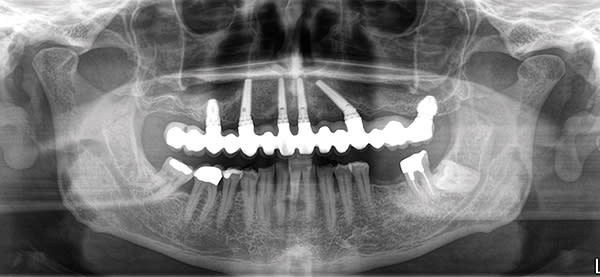
Figure 2
