JingRu Li, PhD; Farah Mirza, BDS, MS; Melissa Nelson, MS; Jessica Foster; Pejmon Amini, DDS; Umar Imtiaz, DDS; and Marilyn Ward, DDS
Abstract: The study objective was to evaluate the effect of two different interdental oral cleaning modalities on gingivitis and plaque following a 4-week period of home use. This was a randomized, parallel, single-blinded study. Subjects were routine manual toothbrush (MTB) users with moderate to severe gingivitis, aged 18 to 65 years. Subjects were required at baseline to have a gingival bleeding score of ≥1 on at least 50 gingival sites per the Gingival Bleeding Index (GBI) and to have an overall plaque score of ≥0.6 per the Rustogi Modified Navy Plaque Index (RMNPI) following a 3- to 6-hour plaque accumulation period. Subjects were randomly assigned to one of three groups based on the oral care cleaning modalities: (1) NON group: MTB alone, (2) IDB group: MTB plus an interdental brush, or (3) MPF group: MTB plus a Philips® Sonicare® Power Flosser with the Quad Stream nozzle. All subjects used the MTB with fluoride toothpaste. Efficacy measures (Modified Gingival Index [MGI], GBI, and RMNPI) and safety were assessed at baseline, 2 weeks, and 4 weeks. The primary efficacy endpoint was the reduction in gingival inflammation from baseline to week 4 as measured by the MGI. A total of 189 subjects were randomized and 186 completed the study. The adjusted mean percent reduction in gingival inflammation from baseline to week 4 was 2.80% for the NON group, 11.32% for the IDB group, and 20.87% for the MPF group. The differences between the MPF group and the NON and IDB groups were statistically significant (P < .0001). In conclusion, use of the MTB with the Philips Sonicare Power Flosser showed statistically significant benefits compared to an MTB alone and an MTB used with an interdental brush in reducing gingival inflammation following 4 weeks of home use.
Although often overlooked, oral health is an important quality-of-life attribute. Lack of proper oral hygiene can lead to gingivitis and periodontal disease due to plaque biofilm buildup.1,2 People with gingivitis and periodontal disease report quality-of-life impacts such as pain, discomfort, tooth loss, and physical appearance changes.3-5 In contrast, treatment of periodontal disease and gingivitis through reduction in plaque and inflammation can lead to an improved quality of life.6
Interproximal surfaces of teeth are hard to reach by toothbrush bristles, thus interdental cleaning devices have been recommended as an adjunct to toothbrushing for the promotion of good oral hygiene. The combination of toothbrushing and interdental cleaning is shown to be more effective in reducing gingivitis and plaque than toothbrushing alone.7,8 Additionally, the combination of toothbrushing and water flossers as interdental cleaning devices has been shown to reduce gingival inflammation and plaque more than manual toothbrushing alone.9,10
Dental professionals commonly customize interdental care recommendations to each patient's unique situation. In general, there is a need for clinical trials that provide more authoritative guidelines on the selection of interdental cleaning aids.11 As such, this study investigates interdental cleaning devices, specifically the Philips® Sonicare® Power Flosser and an interdental brush, and aims to evaluate plaque removal, gingivitis reduction, and safety of these interdental cleaning modalities when used as an adjunct to manual toothbrushing.
Materials and Methods
This was a prospectively planned, randomized, parallel, single-blinded study. The study was reviewed and approved by an accredited Institutional Review Board (IRB00000971, Columbia, Maryland). The study's primary objectives were to evaluate the effect of different oral cleaning modalities on gingivitis, as evaluated by the Modified Gingival Index (MGI),12 following a period of 4 weeks of home use, and to evaluate the safety of test products during this same period. Secondary objectives included an additional gingivitis comparison at a 2-week timepoint and comparisons between the oral cleaning modalities on plaque removal and gingival bleeding at both 2-week and 4-week timepoints. Power analysis for this study was based on the primary efficacy endpoint of MGI reduction at 4 weeks, comparing different cleaning modalities. A sample size of 57 subjects per treatment group was estimated to provide 85% power to detect a difference in reduction in MGI as small as 0.25 using a two-sided t-test after adjusting for multiple comparisons to maintain an overall type I error rate of 0.05 (Hochberg-Bonferroni multiple comparison).
There were three efficacy endpoint measures in this study: the MGI, Gingival Bleeding Index (GBI),13 and Rustogi Modified Navy Plaque Index (RMNPI).14 The MGI and GBI metrics were performed on all evaluable teeth at six sites per tooth, and the RMNPI was recorded at 18 sites per evaluable tooth. The safety endpoints were the adverse changes in the oral cavity upon oral examination and/or subject interview that were "possibly related" or "related" to the test products, adverse events (AEs) that occurred in/around the oral cavity, and any events that were unanticipated adverse device effects.
Subject recruitment included generally healthy individuals that were aged 18 to 65 years, nonsmokers, and regular manual toothbrush users. Subjects were required to have a minimum of 20 scorable teeth (excluding third molars), a minimum average overall RMNPI score of ≥0.6 following a 3- to 6-hour plaque accumulation period, and a gingival bleeding score of ≥1 on at least 50 gingival sites per the GBI. Subjects were excluded if they were regular power toothbrush users or regular users of dental floss or other interdental cleaning techniques.
All subjects in this study used a manual toothbrush (MTB) with or without an additional cleaning modality targeting the interdental space. Study participants were randomized to one of the three treatment groups according to a predefined randomization schedule and stratified by gender. The three treatment groups for the 4-week home use period were: (1) NON group: MTB alone with no interdental cleaning modality, (2) IDB group: MTB plus an interdental brush, or (3) MPF group: MTB plus the Philips Sonicare Power Flosser, used in the clean mode with high intensity along with the Quad Stream nozzle. All subjects were provided with standard fluoride-containing dentifrice to use for the duration of the study and were prohibited from using any other at-home oral hygiene treatments. Subjects were instructed to brush at home with the MTB for 1 minute twice daily for the 4-week period. For the IDB and MPF groups, subjects were instructed to use the interdental cleaning modality once daily in the evening per provided instructions. At each study visit, subjects were required to present with 3 to 6 hours of plaque accumulation. Subjects were provided with a compliance diary to record each interdental cleaning and brushing encounter.
Randomization and subject instruction on device use were performed by designated unblinded study personnel who did not perform any evaluations or assessments related to study endpoints. Efficacy outcomes included the observed response, the reduction from baseline, and the percent reduction from baseline. An analysis of covariance (ANCOVA) model, with baseline score as the covariate, was used to assess treatment response at each visit and compare the response of the MPF group to the NON and IDB groups. All statistical tests were two-sided.
Results
Of the 207 subjects screened for this study, 18 failed screening and 189 were enrolled and randomized to one of the three treatment groups. There were no statistical differences in the distribution of age and gender of subjects between groups (P = .4359 and P = .9511, respectively). Three subjects terminated the study early (one lost to follow-up, one contracted COVID, and one to non-compliance).
Results for the efficacy scores for all treatments at baseline, week 2, and week 4 can be found in Table 1 for the MGI, GBI, and RMNPI. There were no significant differences between treatment groups in the scores at baseline (P > .05) for any of these indices. In addition to Table 1, the adjusted mean percent reduction from baseline in the three indices scores are presented graphically (Figure 1).
Analysis of the percent reduction from baseline showed a statistically significant between-group treatment effect (P < .0001) for all indices at both the week 2 and week 4 timepoints. Pairwise comparisons indicate that the treatment differences between the MPF group and the NON and IDB groups were statistically significant (P < .0001) with the MPF group demonstrating a greater reduction in all indices at the week 2 and week 4 timepoints. At week 4, the improvement for MPF compared to NON was 7.3 times higher for MGI, 6.5 times higher for GBI, and 4.2 times higher for RMNPI. The improvement for MPF compared to IDB was 1.8 times higher for MGI, 2.2 times higher for GBI, and 2.0 times higher for RMNPI.
Twenty-one AEs were reported in the study: six in the NON group, 10 in the IDB group, and five in the MPF group. The AEs were mild in severity. There were 14 AEs that the investigator classified as either "possibly related" or "related" to the study or the study products: two in the NON group, 10 in the IDB group, and two in the MPF group. These AEs were gingival or toothbrush abrasions or irritations.
Discussion and Conclusions
This study of the interdental cleaning modalities cited above supports the conclusion that the adjunctive use of a manual toothbrush and the Philips Sonicare Power Flosser used in the clean mode at the high intensity setting along with a Quad Stream nozzle is safe and showed statistically significant benefits compared to manual toothbrushing alone or manual toothbrushing and the use of an interdental brush in improving the gingival health status and plaque removal of subjects with moderate to severe gingivitis.
The human dentition is a geometrically complex arrangement of hard tissue embedded in a soft tissue and periodontal matrix attaching the teeth to underlying bone structure. Maintaining the health of this dynamic environment is important to preserving the critical roles of mastication, speech, and physical appearance. Dental professionals recommend a daily oral hygiene regimen that removes food debris and dental plaque from the surfaces of teeth. This regimen typically includes cleaning the teeth with a toothbrush and a fluoride-based toothpaste, followed by the use of an interdental cleaning aid. Toothbrushing is generally a well-followed recommendation by most patients, whereas use of an interdental aid may be a less customary part of the oral hygiene regimen.
Manufacturers of oral care products strive to make products that give consumers an array of options for safe and effective oral hygiene. The power flosser category aims to enhance the convenience and efficacy of cleaning the teeth, particularly the interdental areas, through improved fluid-driven access. A pressurized stream of fluid, as delivered by a power flosser, can reach beyond the limits of toothbrush bristles and penetrate areas between teeth. Interdental brushes and string floss can also reach the interdental space but may be met with user resistance. Recent improvements in water-based power flossers have shown to achieve greater benefits to oral health and are more widely appealing to consumers.
In conclusion, the adjunctive use of the Philips Sonicare Power Flosser, used with a Quad Stream nozzle, and a manual toothbrush was shown to provide statistically significant benefits in the reduction of gingival inflammation, gingival bleeding, and plaque, compared to manual toothbrushing alone or manual toothbrushing plus an interdental brush, following 4 weeks of home use. All products used in the study were safe for home use.
Disclosure
This study was sponsored by Philips Oral Healthcare.
About the Authors
JingRu Li, PhD
Senior Clinical Development Scientist, Philips Oral Healthcare, Bothell, Washington
Farah Mirza, BDS, MS
Senior Clinical Development Scientist and Medical-Dental Safety Officer, Philips Oral Healthcare, Bothell, Washington
Melissa Nelson, MS
Associate Director, Biostatistics, Philips Oral Healthcare, Bothell, Washington
Jessica Foster
Senior Clinical Research Associate, Philips Oral Healthcare, Bothell, Washington
Pejmon Amini, DDS
Principal Investigator, Dental Examiner, Silverstone Research Group,
Las Vegas, Nevada
Umar Imtiaz, DDS
Sub Investigator, Dental Examiner, Silverstone Research Group, Las Vegas, Nevada
Marilyn Ward, DDS
Clinical Development Director, Philips Oral Healthcare, Bothell, Washington
References
1. Page RC. Current understanding of the aetiology and progression of periodontal disease. Int Dent J. 1986;36(3):153-161.
2. Seneviratne CJ, Zhang CF, Samaranayake LP. Dental plaque biofilm in oral health and disease. Chin J Dent Res. 2011;14(2):87-94.
3. Broomhead T, Gibson B, Parkinson CR, et al. Gum health and quality of life-subjective experiences from across the gum health-disease continuum in adults. BMC Oral Health. 2022;22(1):512.
4. Petersen PE, Bourgeois D, Ogawa H, et al. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83
(9):661-669.
5. Haag DG, Peres KG, Balasubramanian M, Brennan DS. Oral conditions and health-related quality of life: a systematic review. J Dent Res. 2017;96(8):864-874.
6. Wong LB, Yap AU, Allen PF. Periodontal disease and quality of life: umbrella review of systematic reviews. J Periodontal Res. 2021;56
(1):1-17.
7. Sambunjak D, Nickerson JW, Poklepovic T, et al. Flossing for the management of periodontal diseases and dental caries in adults. CochraneDatabase Syst Rev. 2011;(12):CD008829.
8. Worthington HV, MacDonald L, Poklepovic Pericic T, et al. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database Syst Rev. 2019;4(4):CD012018.
9. Goyal CR, Lyle DM, Qaqish JG, Schuller R. Evaluation of the plaque removal efficacy of a water flosser compared to string floss in adults after a single use. J Clin Dent. 2013;24(2):37-42.
10. Ren X, He J, Cheng R, et al. The efficacy and safety of oral irrigator on the control of dental plaque and gingivitis: a randomized, single-blind, parallel-group clinical trial. Int J Environ Res Public Health. 2023;20(4):3726.
11. Richards D. The effectiveness of interproximal oral hygiene aids. Evid Based Dent. 2018;19(4):107-108.
12. Lobene RR, Weatherford T, Ross NM, et al. A modified gingival index for use in clinical trials. Clin Prev Dent. 1986;8(1):3-6.
13. Van der Weijden GA, Timmerman MF, Nijboer A, et al. Comparison of different approaches to assess bleeding on probing as indicators of gingivitis. J Clin Periodontol. 1994;21(9):589-594.
14. Rustogi KN, Curtis JP, Volpe AR, et al. Refinement of the Modified Navy Plaque Index to increase plaque scoring efficiency in gumline and interproximal tooth areas. J Clin Dent. 1992;3(suppl C):C9-C12.
Figures and Images
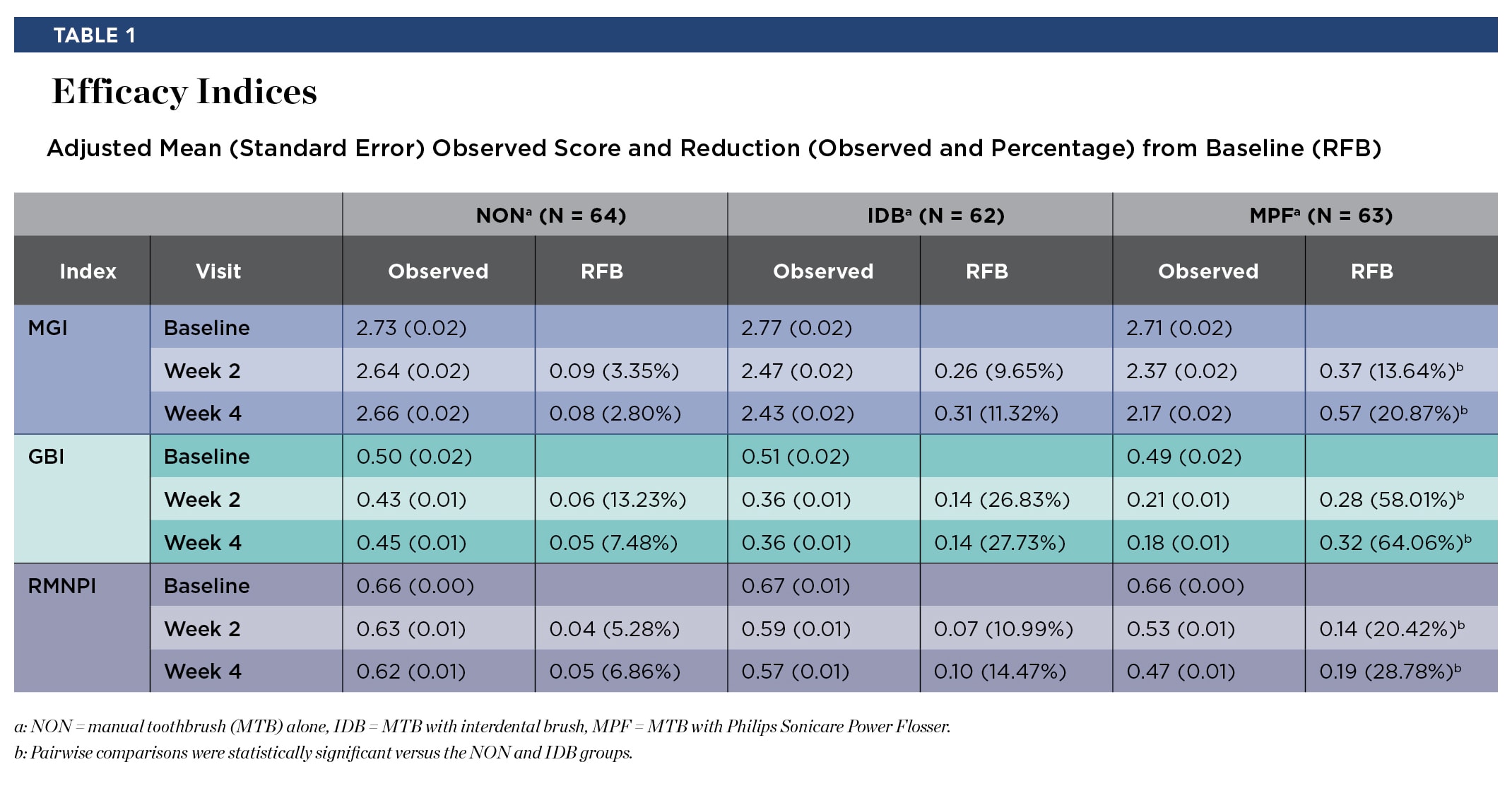
Table 1

Figure 1
