Thomas J. Lambert, DDS
Abstract: Objective: This practice-based case series evaluated the effects of the Oral-B® iO™ oscillating-rotating (O-R) electric toothbrush with the novel Targeted Clean™ brush head as part of a home care regimen on the health of the tissues surrounding implant-borne fixed restorations. Methods: Eight generally healthy, nonsmoking patients with peri-implant mucositis in at least one implant site and moderate-to-high plaque levels who had not had a professional cleaning in 3 months and were not currently using an O-R toothbrush were recruited from the author's practice. Fixed implant restorations on these eight patients were evaluated for plaque and gingival inflammation (erythema, swelling, and bleeding on probing [BOP]). In collaboration with the dental hygiene team, the patients were introduced to specific protocols for implant maintenance utilizing the Oral-B iO O-R brush and the Targeted Clean brush head. After 6 weeks the patients were re-evaluated. Clinical findings with photographs and probing as well as the impact of the intervention on each patient's motivation and compliance in maintaining oral hygiene at home were recorded. Results: After 6 weeks, implant sites with baseline peri-implant mucositis demonstrated no BOP or other signs of inflammation and reduced plaque scores. The patients' home care compliance and motivation to maintain effective oral hygiene around their implants saw a substantial improvement. Conclusions: The Oral-B iO O-R electric toothbrush with the novel Targeted Clean brush head, used as part of a home care regimen, markedly reduced peri-implant mucositis around fixed implant restorations among all eight patients in this case series. Key factors were the patient owning their disease pattern and the doctor/hygienist collaboration and use of education protocols to help improve the patients' home care compliance and motivation.
The use of dental implants as a sustainable restorative treatment has grown exponentially over the past two decades. The Dental Implants Global Market Report 2021 expected growth to $4.5 billion with a compound annual growth rate of 8.7% as more patients opt for this treatment modality to replace fractured and periodontally involved teeth with questionable prognoses.1 Additionally, a growing number of completely edentulous patients are turning to full-arch fixed implant restorations as a solution for their esthetic and functional concerns, which in the United States alone has seen an increase in implant prevalence from 0.7% in 1999-2000 to 5.7% in 2015-2016.2
The success of an implant restoration is fundamentally dependent on effective planning, placement of the implant, and restoration, but the implant's long-term management then shifts to the hygienist and the ability of the patient to perform effective self-care at home. Historically, dental and dental hygiene education focused on the health of the periodontium, specifically the tissues surrounding the natural tooth. Little to no time was spent studying the health of the tissues surrounding the implant restoration itself. Today, with more fixed implant restorations in the mouths of patients than in the past, clinicians may often notice inflammation and bleeding from the tissues surrounding the implants. This peri-implant mucositis is frequently due to suboptimal plaque control around the implant and the surrounding tissues.3 Left untreated, with ongoing poor plaque control, peri-implant mucositis can progress to peri-implantitis and potential loss of the implant.4 Furthermore, the association between periodontal disease and systemic conditions, such as cardiovascular disease and diabetes, is well documented in the literature.5
The World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions concluded the standard of care for managing peri-implant mucositis is mechanical biofilm control.7 In addition, Clinical Practice Guidelines from the American College of Prosthodontists, which are based on findings from two comprehensive systematic reviews, recommend that patients with implant-borne restorations be educated about brushing twice daily and the use of oral hygiene aids, including water flossers, air flossers, interdental cleaners, and electric toothbrushes, as part of at-home maintenance.8 Difficulties often occur when instructing patients to clean around narrow-neck implants with bulbous crowns. Additionally, fully edentulous patients with implant-supported fixed final prostheses are presented with unique challenges in removing plaque and biofilm from under and around the prosthesis and implants.
The type of toothbrush patients use along with their brushing behaviors are critical factors in their ability to achieve optimal plaque control. Electric toothbrushes have been consistently shown as superior to manual toothbrushes in removing plaque biofilm, reducing bleeding, and increasing retention of teeth as evidenced by systematic reviews, meta-analyses,9,10 and multi-year observational research.11There are two main categories of electric toothbrushes. Oscillating-rotating technology, characterized by filaments continuously rotating in one direction and then another, was first introduced in the 1990s by Oral-B to maximize disruption and removal of plaque biofilm. Sonic toothbrushes are another common class of electric toothbrushes. They typically have a larger head size and vibrate side to side at a high rate of speed and emit a harmonic tone. Among electric toothbrushes, oscillation-rotation technology has demonstrated superior gingival health benefits compared to other electric toothbrush technologies, including sonic,9 while findings on its efficacy among patients with implants and implant-supported fixed prostheses have shown significantly improved plaque control and gingival health.12-16
Oral-B iO and Targeted Clean Brush Head
In 2020, the author was invited to participate in a global practice-based program evaluating the new Oral-B iO toothbrush with Targeted Clean brush head with a select group of his implant patients. The Oral-B iO is a next-generation oscillating-rotating (O-R) electric toothbrush. It has the same clinically proven O-R motion as previous models, but the brush has been completely redesigned. Procter & Gamble researchers and engineers spent 7 years developing the Oral-B iO toothbrush, which is driven by a series of magnets, described as a "linear magnetic drive system" that directs energy to the bristle tips and also results in micro-vibrations that produce an enhanced brushing experience.17
The smart pressure sensor is a tremendous advancement for patients by providing optimal pressure feedback when flashing green, and flashing red when it senses excessive pressure; also, the user has a choice of colors that can be customized to indicate too little pressure. The organic light-emitting diode (OLED) smart display has up to seven brushing modes and provides personalized coaching and motivation. The Oral-B app provides real-time tracking to promote thorough brushing and proper pressure and increase patient motivation and compliance. The personalized feel of the brush is designed for patients to take ownership of their own dental health and be motivated to achieve excellent outcomes.
Redesigned Oral-B brush heads include the Ultimate Clean brush head with an innovative tuft-in-tuft bristle pattern for enhanced reach and the Gentle Care brush head with the manufacturer's smallest-diameter filaments. The newest brush head is the Targeted Clean brush head (Figure 1), designed for effective plaque control around implants, braces, misaligned teeth, and other areas that require special focus.
Randomized controlled studies, ranging from single-use evaluations to 6-month trials, show the Oral-B iO technology provides significantly greater gingival health and plaque removal benefits compared to manual and sonic toothbrush controls.18-21
Case Series Overview and Practical Implications
This case series was designed to evaluate the impact of the Oral-B iO toothbrush, when used as part of a home care regimen, on dental implant health in a group of patients with fixed implant restorations over a 6-week period. The selection criteria included patients with peri-implant mucositis, good general health, and who were nonsmokers. Patients demonstrated pre-existing moderate to high plaque levels and had not had a professional cleaning in 3 months.
There were six females and two males; average age was 56.9 years (range: 35 to 66 years). This group of patients had inadequate compliance with oral hygiene, and they were currently not brushing with an O-R toothbrush. The group consisted of five patients with at least one single implant and crown restoration, one patient with a fixed implant four-unit implant-retained bridge, and two patients with maxillary and mandibular full-arch implant-supported fixed final prostheses. The average implant age was 2.8 years (all were 1 to 5 years in age). The occlusion in all patients was balanced with no lateral or protrusive inferences and light to minimal contact in centric occlusion. Six patients were currently using a sonic electric toothbrush and two were using manual toothbrushes.
The initial evaluation consisted of bleeding scores (yes-no), plaque levels (low-moderate-high), gingival inflammation assessments (yes-no), and intraoral photographs. An experienced dental hygienist in the author's practice was an integral part of this study. Her role was to assess the current techniques patients were using at home by asking them to describe their home care routine in detail. Additional questioning helped determine the motivational level of each patient (low-moderate-high) and educate the patient, using the so-called "co-discovery" strategy outlined in Figure 2.22
Each patient was provided their own Oral-B iO with an Ultimate Clean brush head, Gentle Care brush head, and Targeted Clean brush head. The dental hygienist reviewed the features of the Oral-B iO, including the pressure sensor, smart display, and app. With the patient holding a mirror, the iO brush with the Ultimate Clean brush head was demonstrated in the patient's mouth showing proper angulation and movement across the arch. The Targeted Clean brush head was placed on the Oral-B iO and demonstrated in the mouth with proper angulation around implants and areas that require special focus (Figure 3 and Figure 4). Patients who were currently using interproximal brushes and aids were asked to stop using them and replace them by cleaning those areas using the Targeted Clean brush head. Flossing technique was demonstrated for patients with intact dentitions.
Patients were instructed to first use the Oral-B iO brush for 2 minutes. This was to be followed with the Targeted Clean brush head used around each dental implant and other areas specifically recommended by the dental hygienist. Patients were dispensed a 0.07% cetylpyridinium chloride (CPC) rinse (Crest® Pro-Health Mouthrinse) and instructed to rinse their entire mouth twice daily for 60 seconds. A 0.454% bioavailable stannous fluoride dentifrice (Crest® Pro-Health Gum Detoxify) was dispensed, and the patients were instructed to brush their entire dentition three times daily while using the Oral-B iO, the Targeted Clean brush head, and the app.
Two patients presented with maxillary and mandibular full-arch fixed implant restorations. Both were using a water flosser, bridge threaders, and manual toothbrushes. As with the other patients, the dental hygienist instructed them on the use of the Oral-B iO with Ultimate Clean brush head for the prosthesis itself. The Targeted Clean brush head was also demonstrated to clean under the prosthesis and around the implants (Figure 5). The Targeted Clean brush head was positioned on the facial, lingual, and palatal aspects of the prosthesis as the patient observed the brush movement around each implant and under the prosthesis itself. The patients were dispensed the same CPC rinse and stannous fluoride dentifrice and directed to use them following the same instructions given the first group of patients.
Clinical and Behavioral Observations
2-Week Evaluation
All of the patients returned for a 2-week evaluation whereby their progress was assessed and adjustments were made to their home care routine. Bleeding and inflammation were reduced in each patient. Patients were asked what they liked and did not like about their brushing experience and which areas in their mouth they felt improvement was needed. The author and hygienist carefully observed the patients' use of their brush in their mouth. The proper positioning of the Targeted Clean brush head was reviewed to ensure proper plaque removal around implants and other critical areas as recommended by the dental hygienist.
The pressure sensor and the app helped reveal that several of the patients were brushing with insufficient pressure. One patient stated, "because of my recession I always felt like I was brushing too hard." The Gentle Care brush head and the Sensitive setting were then recommended for this patient. The option of two brush heads, the app, and the choice of power setting changed this patient's behavior and motivation in a positive direction.
6-Week Evaluation
At the 6-week evaluation, the six patients who had a mixture of natural teeth and dental implants demonstrated no bleeding and no inflammation around their implants. Plaque accumulation throughout their mouths was minimal. All patients displayed notably improved compliance and motivation and were pleased with the overall improvement in their dental health. Details of the patient evaluation are shown in Table 1.
Featured Patients
Patient No. 1 had presented with a full-arch smile makeover. Implant No. 10 in this patient had BOP and inflammation around the implant (Figure 6 and Figure 7). At the 6-week evaluation of the tissues of implant No. 10 there was no BOP and the patient had returned to health (Figure 8 and Figure 9). She was excited to learn that her new home care protocols with the Oral-B iO brush and Targeted Clean brush head had made a positive impact on the health of her mouth, stating that she "loved my Oral-B iO brush so much" that often times she brushed for 5 minutes and was "so happy" that her gums no longer bled and that her mouth was healthy and clean.
Patient No. 4 had presented with maxillary and mandibular fixed implant-supported prostheses. Upon removal of the prosthetics, inflammation, including BOP, was noted around the implant abutments. The prosthesis was cleaned (Figure 5), abutments debrided, and then torqued back into place. The patient returned following 6 weeks of using the Oral-B iO brush and the Targeted Clean brush head. The prosthetics were removed. Minimal debris was evident around the prosthesis and no BOP or other signs of gingival inflammation were present. The patient was highly motivated and stated, "This is the only powered brush I have found to actually reach under my teeth and clean the implants. My mouth feels fresh, clean, and healthy after using the Targeted Clean brush head."
Observations
A critical step in the success of these cases is related to the author's team's mission in dentistry to "educate and guide our patients toward the healthiest and most beautiful smile possible." The key word in this mission is "educate." Time management is typically a critical concern in dental offices, and all too often very little time is allocated for oral hygiene education. When educating the patients in this study, the team began by helping them understand why oral health is important, addressing the question, "Why should I change what I have always been doing?"
The "co-discovery" journey (Figure 2) starts with the dental hygienist handing the patient a mirror and probing an area around an implant or tooth with bleeding. An intraoral photograph is taken and shown in full screen on the monitor above the patient. We now engage the patient in the process by asking if they can see the bleeding. When they respond affirmatively, our response is always, "Healthy gums do not bleed." We then ask if they are aware that gum disease is associated with systemic disease, such as diabetes and heart disease.5 This typically gets the patient's full attention.
At this point the patient is beginning to "own" their dental disease. They will often ask, "I don't like this; what can I do about it?" Once the patient understands their disease pattern and owns their problem, then and only then are they ready for a solution. The patient is now ready to learn and be open to adopting oral hygiene instruction, which should include personalized home care recommendations. Interactive electric toothbrushes, such as the one used in this study, provide a range of brushing modes and heads for specific patient needs, and they can be recommended with a dentifrice, mouthrinse, and/or interdental cleaner for an individualized oral hygiene routine. The Oral-B iO Test Drive program, in which the patient has the opportunity to experience the toothbrush in the operatory under the guidance of a dental professional, is an example of a hands-on method to facilitate oral hygiene adoption.23 The co-discovery process is well worth the investment in time and can lead to better outcomes for patients, as demonstrated by this case series.
It is important to note that this was practice-based research involving case studies, not a single-variable clinical study; therefore, the author cannot determine the relative contribution of individual products or the co-discovery process to the outcomes. However, these findings are consistent with results from randomized controlled trials showing significant oral health benefits for regimens similar to the one evaluated here and for oral hygiene instructional methods.24-26 Exploration of the relative benefit of each factor would require investigation in randomized controlled trials.
Conclusions
The Oral-B iO oscillating-rotating electric toothbrush with the new Targeted Clean brush head, used as part of an oral hygiene regimen, was shown to notably reduce peri-mucositis around implants, implant-borne restorations, or prostheses. A major factor was the patient owning their disease pattern through the co-discovery process and having customized home care instruction from the dental hygienist. The doctor/hygienist collaboration and education protocols dramatically improved patients' home care compliance and motivation.
Acknowledgment
The author thanks Lori Totten, RDH, for her important role in this case series.
Disclosure
This case series was supported by Procter & Gamble. Dr. Lambert has done consulting work for Procter & Gamble.
About the Author
Thomas J. Lambert, DDS Lecturer, Author, and Practitioner of Restorative and Implant Dentistry in Grand Rapids, Michigan
References
1. The Business Research Company. Dental Implants Global Market Report 2021: COVID 19 Growth and Change to 2030. Report Linker website. May 2021. https://www.reportlinker.com/p06071073/?utm_source=GNW. Accessed March 8, 2022.
2. Elani HW, Starr JR, Da Silva JD, Gallucci GO. Trends in dental implant use in the U.S., 1999-2016, and projections to 2026. J Dent Res. 2018;97(13):1424-1430.
3. Lee CT, Huang YW, Zhu L, Weltman R. Prevalences of peri-implantitis and peri-implant mucositis: systematic review and meta-analysis. J Dent. 2017;62:1-12.
4. Romandini M, Lima C, Pedrinaci I, et al. Prevalence and risk/protective indicators of peri-implant diseases: a university-representative cross-sectional study. Clin Oral Implants Res. 2021;32 (1):112-122.
5. Scientific American. How poor oral health fosters systemic disease. Scientific American website. https://www.scientificamerican.com/custom-media/healthy-mouth-healthy-body/how-poor-oral-health-fosters-systemic-disease/. Accessed March 8, 2022.
6. Berglundh T, Armitage G, Araujo MG, et al. Peri-implant diseases and conditions: consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. 2018;45(suppl 20):S286-S291.
7. Jepsen S, Berglundh T, Genco R, et al. Primary prevention of peri-implantitis: managing peri-implant mucositis. J Clin Periodontol. 2015;42(suppl 16): S152-S157.
8. Bidra AS, Daubert DM, Garcia LT, et al. Clinical practice guidelines for recall and maintenance of patients with tooth-borne and implant-borne dental restorations. J Prosthodont. 2016;25(suppl 1):S32-S40.
9. Grender J, Adam R , Zou Y. The effects of oscillating-rotating electric toothbrushes on plaque and gingival health: a meta-analysis. Am J Dent. 2020;33(1):3-11.
10. Yaacob M, Worthington HV, Deacon SA, et al. Powered versus manual toothbrushing for oral health. Cochrane Database Syst Rev. 2014;2014(6):CD002281.
11. Pitchika V, Pink C, Völzke H et al. Long-term impact of powered toothbrush on oral health: 11-year cohort study. J Clin Periodontol. 2019;46(7):713-722.
12. Allocca G, Pudylyk D, Signorino F, et al. Effectiveness and compliance of an oscillating-rotating toothbrush in patients with dental implants: a randomized clinical trial. Int J Implant Dent. 2018;4(1):38.
13. Biesbrock AR, et al. Plaque image analysis of combination oral hygiene with dental implants [abstract]. J Dent Res. 2013;92(spec iss A):Abstract 2590.
14. Maeda T, Mukaibo T, Masaki C, et al. Efficacy of electric-powered cleaning instruments in edentulous patients with implant-supported full-arch fixed prostheses: a crossover design. Int J Implant Dent. 2019;5(1):7.
15. Rasperini G, Pellegrini G, Cortella A, et al. The safety and acceptability of an electric toothbrush on peri-implant mucosa in patients with oral implants in aesthetic areas: a prospective cohort study. Eur J Oral Implantol. 2008;1(3):221-228.
16. Vanderkerckhove B, Quirynen M, Warren PR, et al. The safety and efficacy of a powered toothbrush on soft tissues in patients with implant-supported fixed prostheses. Clin Oral Investig. 2004;8(4):206-210.
17. Adam R. Introducing the Oral-B iO electric toothbrush: next generation oscillating-rotating technology. Int Dent J. 2020;70(suppl 1):S1-S6.
18. Goyal CR, Adam R, Timm H, et al. A 6-month randomized controlled trial evaluating a novel smart-connected oscillating-rotating toothbrush versus a smart-connected sonic toothbrush for the reduction of plaque and gingivitis. Am J Dent. 2021;34(1):54-60.
19. Adam R, Erb J, Grender J. Randomized controlled trial assessing plaque removal of an oscillating-rotating electric toothbrush with micro-vibrations. Int Dent J. 2020;70(suppl 1):S22-S27.
20. Grender J, Goyal CR, Qaqish J, Adam R. An 8-week randomized controlled trial comparing the effect of a novel oscillating-rotating toothbrush versus a manual toothbrush on plaque and gingivitis. Int Dent J. 2020;70(suppl 1):S7-S15.
21. Adam R, Goyal CR, Qaqish J, Grender J. Evaluation of an oscillating-rotating toothbrush with micro-vibrations versus a sonic toothbrush for the reduction of plaque and gingivitis: results from a randomized controlled trial. Int Dent J. 2020;70(suppl 1):S16-S21.
22. Hewell K. Sneak peek: case acceptance bootcamp with Adam McWethy. Spear website. September 3, 2021. https://www.speareducation.com/spear-review/2021/08/case-acceptance-dental-practice-bootcamp-adam-mcwethy. Accessed March 24, 2022.
23. Oral-B Test Drive Power Brush Trial Program Kit Regulation Number: 21 CFR 872.6865 Toothbrush, Powered Regulatory Class: I Product Code: JEQ. Dated: August 14, 2014. Received: August 15, 2014.
24. Zini A, Mazor S, Timm H, et al. Effects of an oral hygiene regimen on progression of gingivitis/early periodontitis: a randomized controlled trial. Can J Dent Hyg. 2021;55(2):85-94.
25. Adam R, Grender J, Timm H, et al. Anti-gingivitis and anti-plaque efficacy of an oral hygiene system: results from a 12-week randomized controlled trial. Compend Contin Educ Dent. 2021;42(9):e1-e4.
26. Holloway JA, Davies M, McCarthy C, et al. Randomised controlled trial demonstrating the impact of behaviour change intervention provided by dental professionals to improve gingival health. J Dent. 2021;115:103862.
Figures and Images

Figure 1
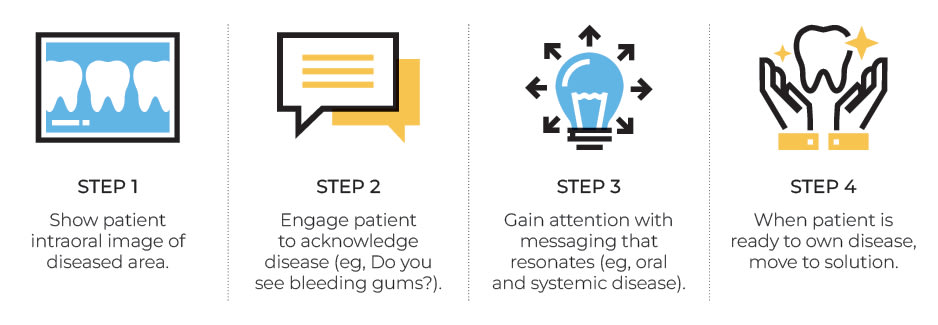
Figure 2

Figure 3

Figure 4

Figure 5

Figure 6

Figure 7

Figure 8

Figure 9

Table 1
