Julie Grender, PhD; C. Ram Goyal, DDS; Jimmy Qaqish, BSc; Hans Timm, PhD; and Ralf Adam, PhD
Abstract: Objective:This study compared the gingivitis and plaque reduction efficacy of a novel smart-connected oscillating-rotating (O-R) electric toothbrush with micro-vibrations, used in Sensitive mode with an extra gentle ("sensitive") brush head, to the efficacy of a soft manual toothbrush. Methods:This was a 12-week, examiner-blind, two-treatment, parallel-group clinical trial with 100 adult subjects (N = 100) having evidence of gingivitis and plaque at baseline. Subjects were randomly assigned to use either the O-R electric rechargeable toothbrush (Oral-B® iO™ with Oral-B Gentle Care brush head) or the soft manual toothbrush (Oral-B Indicator). Gingivitis was assessed with the modified gingival index (MGI) and the gingival bleeding index (GBI). Plaque was assessed with the Rustogi modification of the navy plaque index (RMNPI). Patients were classified as having a "healthy" (<10% bleeding sites) or "not healthy" (≥10% bleeding sites) gingival case status according to the criteria of the American Academy of Periodontology and the European Federation of Periodontology. Efficacy assessments and oral soft-tissue examinations were conducted before brushing at baseline, week 1, and week 12. The baseline assessment included both pre- and post-brushing plaque evaluations to evaluate single-use plaque removal efficacy. Results:All 100 subjects completed the trial. Subjects had a mean age of 49.1 years; 72% were females. The O-R brush group had a significantly higher percentage of subjects who transitioned from "not healthy" to "healthy" gingival case status than did the manual brush group (at week 12: 92% vs 24%; P< .001). At week 12, the O-R brush group also demonstrated a significantly greater (P< .001) mean number of bleeding sites reduced (23 vs 7), mean MGI reduction (0.45 vs 0.17), and mean GBI reduction (0.18 vs 0.06). Plaque reduction for the O-R brush group was also significantly greater (P≤ .009) than for the manual brush group for whole mouth, gingival margin, and interproximal region, from day 1 (single use) through 12 weeks. Both brushes were well tolerated.Conclusion:The novel O-R toothbrush with micro-vibrations used in Sensitive mode with an extra gentle brush head provided significantly greater gingivitis and plaque reduction than did a manual toothbrush over 12 weeks.
Gingivitis, the first stage of periodontal disease, is prevalent globally and affects more than 90% of American adults.1 The condition stems from an inflammatory reaction to bacteria in dental plaque and results in gingival bleeding, redness, and swelling.2 Gingivitis can negatively impact oral hygiene because mechanical plaque removal from inflamed gingiva may be painful. This was shown in a recent systematic review that found an association between gingivitis and pain along with difficulties in toothbrushing.3 Patients might, therefore, avoid thorough hygiene in areas with gingivitis, worsening gingival inflammation and bleeding.
Fortunately, gingivitis can be reversed with appropriate treatment, including daily plaque control via toothbrushing.4-7 There is abundant evidence demonstrating the benefits of electric toothbrushes over manual toothbrushes for plaque removal and gingivitis reduction,8,9 with studies specifically showing efficacy advantages for oscillating-rotating (O-R) electric brush technology over manual and other electric toothbrush (eg, sonic) controls.8-13 In a recent meta-analysis that analyzed gingival bleeding data using gingivitis case definitions from the World Workshop on the Classification of Periodontal and Peri-implant Diseases and Conditions,14 significantly more subjects with "localized" (10% to 30% bleeding sites) or "generalized" (more than 30% bleeding sites) gingivitis who used an O-R electric toothbrush transitioned to "healthy," defined as less than 10% bleeding sites, compared to manual and sonic toothbrush controls.11
The demand for effective plaque removal that also delivers a brushing experience that is personalized to the user's sensory needs, such as in areas that are painful due to gingivitis, has led to the development of specialized toothbrushes and features. These include soft tapered bristles, modified brush head designs, and slower "sensitive" modes for electric toothbrushes. For optimal oral health, these options must be not only gentle but also effective in reducing plaque and gingivitis.
A novel smart-connected O-R electric toothbrush with micro-vibrations (Oral-B iO) was recently introduced with up to two Sensitive modes, depending on the model, and a Gentle Care brush head for gentle-feel cleaning. The brush, which employs clinically proven O-R technology,8,11-13,15,16 has a linear magnetic drive system and has been demonstrated to be safe and more effective than manual or sonic toothbrush controls in studies ranging from single use to 6 months when used in Daily Clean mode with the Ultimate Clean brush head.17-22 The present study was conducted to evaluate the performance of the novel O-R toothbrush in the removal of plaque and reduction of gingivitis among subjects with localized or generalized gingivitis when the brush was used in Sensitive mode with the Gentle Care brush head.
Methods and Materials
Ethical Aspects
The study was conducted in compliance with the Declaration of Helsinki and the Tri-Council Policy Statement (2nd Edition): Ethical Conduct for Research Involving Humans (2010) and conformed to the standards of Good Clinical Practices-Clinical Investigation of Medical Devices for Human Subjects (ISO) and those of the International Council for Harmonization. The study was registered in the ISRCTN Registry (ISRCTN77960012). Institutional review and approval of the protocol were obtained (Veritas IRB, Inc., Ref# 2020-2303-2707-3). Subjects were recruited by All Sum Research Center. All subjects provided written informed consent.
Study Population
All subjects were healthy adults who habitually used a manual toothbrush and who had at least 16 natural, scorable teeth. Qualifying subjects had a baseline whole-mouth modified gingival index (MGI)23 score of at least 1.75 but not more than 2.5, a whole-mouth pre-brushing Rustogi modification of the navy plaque index (RMNPI)24 score greater than 0.5, and at least 20 but not more than 90 bleeding sites (sites with a gingival bleeding index [GBI]25 score of 1 or 2). Exclusion criteria included a need for antibiotics before dental procedures; grossly carious teeth; severe periodontal disease; active treatment for periodontitis, cancer, or a seizure disorder; use of an antibiotic or chlorhexidine mouthrinse within the previous 2 weeks; oral or periodontal surgery within the previous 2 months; presence of orthodontic appliances, removable partial dentures, or peri/oral piercings; presence of a pacemaker or other implanted device; current or anticipated pregnancy; or nursing. All subjects agreed to avoid elective dentistry, use of non-study oral hygiene products, and participation in all other oral care studies.
Clinical Assessment
The same blinded examiner assessed gingivitis and plaque for each subject at each visit. Clinical information was recorded for all scorable teeth, excluding third molars, crowns, implants, bridges, or teeth with orthodontic appliances or restorations covering ≥50% of the tooth surface.
Gingivitis was evaluated according to the MGI and GBI.23,25 MGI scores (six per tooth) ranging from 0 (normal) to 4 (severe inflammation) were assigned to the buccal and lingual marginal gingival regions and to the interdental papillae. GBI scores of 0 (absence of bleeding after 30 seconds), 1 (bleeding observed after 30 seconds), or 2 (immediate bleeding observed) were assigned to the buccal, mesial/distal, and lingual areas of the teeth after standardized probing with a 0.5 mm-tipped periodontal probe. Whole-mouth scores for each index were calculated by dividing the total score by the number of scorable sites examined. Patients were classified as having a "healthy" (<10% bleeding sites) or "not healthy" (generalized and localized gingivitis, ≥10% bleeding sites) gingival case status according to the criteria of the American Academy of Periodontology and the European Federation of Periodontology.14
Plaque was evaluated according to the RMNPI.24 Plaque was scored on the buccal and lingual surfaces of each scorable tooth (nine sites per surface, for a total of 18 sites per tooth). Plaque was scored as absent (0) or present (1), and a mean plaque index (MPI) was calculated by dividing the total number of tooth areas with plaque by the number of tooth areas scored. Separate MPI scores were calculated to reflect the plaque status of the whole mouth, gingival margin, interproximal region, and lingual region.
Investigational Products
Subjects in the electric O-R brush group received kit boxes containing a rechargeable electric O-R toothbrush handle (Oral-B® iO, OP020), a charger, and a sensitive brush head (Oral-B® Gentle Care, OR017; Figure 1). Subjects in the O-R group had the option of using the Oral-B® iO app. Subjects in the control group received a kit box containing a manual toothbrush (Oral-B®Indicator35 soft manual toothbrush, OM003). All kit boxes contained 1100 ppm sodium fluoride dentifrice (Crest Cavity Protection). All study products were manufactured by The Procter & Gamble Company (us.pg.com).
Study Design
This was a 12-week, single-center, examiner-blind, two-treatment, parallel-group, randomized, controlled clinical trial.Assessments were conducted at baseline (day 1), week 1, and week 12. Subjects were instructed to refrain from eating, drinking, chewing gum, or using lozenges, mints, or tobacco for 4 hours prior to each visit and to refrain from all oral hygiene procedures for 12 hours prior to each visit.
At the baseline visit, subjects provided medical history and demographic information. Inclusion/exclusion criteria were reviewed and documented. Subjects then received a pre-brushing oral examination and evaluations of MGI and GBI, all administered by an experienced examiner.18,19,22 Next, the same examiner used Chrom-O-Red® erythrosine FD&C red 3 disclosing solution (Germiphene Corp., germiphene.com) to disclose plaque before performing an RMNPI assessment.
Qualifying subjects were stratified according to tobacco use (present or absent), number of bleeding sites (≤30 vs >30), and mean scores for whole-mouth pre-brushing MGI (≤2.1 vs >2.1) and RMNPI (≤0.62 vs >0.62). A balance and assignment procedure was used to randomly assign stratified subjects to one of two treatment groups. Following group assignment, subjects received their study products in a protected area to ensure that the examiner remained blind to treatment product.
Subjects were instructed to use their products at home twice per day (morning and evening) throughout the study. Subjects in the O-R brush group were directed to operate their brush in Sensitive mode and brush for 2 minutes at each use. Subjects in the manual brush group were directed to brush their teeth in their customary manner.
Subjects in the O-R toothbrush group were provided with assistance in downloading and connecting the Oral-B app if they desired to do so. All subjects were given supervised instructions for their assigned product use and asked to practice using the product in front of a mirror at the site. After this initial use, each subject received a second oral examination followed by plaque disclosure and RMNPI assessment from the same examiner.
At the week 1 visit (±2 days) and the week 12 visit (±3 days), subjects returned to the site and continuance criteria were assessed and recorded. The same examiner conducted a pre-brushing oral examination followed by MGI and GBI assessments, plaque disclosure, and RMNPI assessment, in that order.
Visual examination of the oral cavity/perioral area and dentition/restorations was conducted to assess oral soft tissues and hard tissues, respectively. Any new abnormal finding that was noted after product distribution or that was previously noted and increased in severity during the treatment period was recorded as an "adverse event." All self-reported adverse events were recorded. Any whole-body adverse events potentially related to product use were collected.
Sample Size and Statistical Analysis
Using data from a similar study, power analyses were conducted with α = 0.05, using a two-sided test and a sample size of 50 subjects per group. This sample size provided at least 90% power to detect a between-treatment difference of 3.5 in the number of bleeding sites and at least 90% power to detect a difference of 0.036 units in the whole-mouth mean RMNPI score.
The percentages of subjects classified as having "healthy" (<10% bleeding sites) and "not healthy" (≥10% bleeding sites) gingival case status were computed and compared between treatment groups using a chi-square test. The odds ratio of transitioning from "not healthy" to "healthy" was calculated at week 1 and week 12.
Statistical analyses for gingivitis efficacy were based on change from baseline of whole-mouth average MGI score, GBI score, and number of bleeding sites (baseline minus week 1 and baseline minus week 12). Treatment differences in whole-mouth average gingivitis reduction at week 1 and week 12 were performed using analyses of covariance (ANCOVA). Separate analyses were performed for each gingivitis endpoint, with the respective baseline gingivitis score as the covariate. Week 12 was the most important timepoint and MGI was the primary endpoint. Within-treatment differences from baseline gingivitis scores were tested versus zero using paired-difference t tests.
Whole-mouth, gingival margin, and interproximal plaque reductions after a single brushing at the baseline visit (pre-brushing minus post-brushing) were each analyzed for treatment differences using an ANCOVA model with the respective pre-brushing RMNPI score as the covariate.
Multiple-brushing plaque reduction efficacy analyses were based on the change from baseline of the pre-brushing whole-mouth average RMNPI score (baseline pre-brushing minus week 1 and baseline pre-brushing minus week 12). Treatment differences were analyzed using an ANCOVA model with baseline pre-brushing whole-mouth average RMNPI score as the covariate. An analysis of variance (ANOVA) was used to analyze the gingival margin and interproximal RMNPI endpoints since the baseline values for these endpoints were very similar across all subjects. Within-treatment differences from baseline RMNPI scores were tested versus zero using paired-difference t tests.
Gingivitis and plaque on the lingual surfaces of teeth were analyzed separately as described above. All treatment comparisons were considered two-sided with an α = 0.05 significance level.
Results
Study Population
From among 100 subjects screened, all qualified and completed the study. The study population consisted of 72 females and 28 males, with a mean age (standard deviation, SD) of 49.1 (11.07) years (Table 1).
Transition to Gingival Health
At baseline all subjects presented in a state of localized or generalized gingivitis, classified as having a "not healthy" gingival case status per inclusion criteria (≥10% bleeding sites or >20 bleeding sites), with the number of bleeding sites ranging from 20 to 78. The percentage of subjects who transitioned from "not healthy" to "healthy" gingival case status was significantly greater (P < .001) in the O-R brush group than in the manual brush group at week 1 (20% vs 6%) and week 12 (92% vs 24%) (Table 2). The odds ratio of transitioning from "not healthy" to "healthy" was 3.9 times greater (95% CI, 1.008-15.220) at week 1 and 36.4 times greater (95% CI, 10.855-122.173) at week 12 for the O-R brush group than for the manual brush group.
Gingivitis Reduction Efficacy
The baseline mean number of bleeding sites, MGI score, and GBI score did not differ significantly between groups, including whole mouth and lingual surfaces (P ≥ .670). At week 1 and week 12, both groups exhibited significant reduction from baseline in all measures of gingivitis (P < .001 for all). The O-R brush produced significantly greater reductions in mean number of bleeding sites, whole-mouth MGI, and whole-mouth GBI at week 1 and week 12 than did the manual brush (week 12, by 3.2 times for number of bleeding sites, by 2.7 times for MGI, and by 2.9 times for GBI; P< .001 for all measures). Figure 2 displays the percentage of subjects with bleeding per site at baseline, week 1, and week 12. Measures of gingivitis were similarly reduced at the lingual subregions (week 12, by 4.3 times for lingual surface number of bleeding sites, by 2.4 times for lingual surface MGI, and by 3.9 times for lingual surface GBI; P< .001 for all measures) (Table 3).
Plaque Reduction Efficacy
Baseline whole-mouth, gingival margin, interproximal region, and lingual surface pre-brushing RMNPI scores did not differ significantly between groups (P≥ .187). After a single use, the O-R brush produced significantly greater adjusted mean reductions for whole-mouth, gingival margin, interproximal, lingual, lingual surface gingival margin, and lingual surface interproximal RMNPI scores (P < .001) than the manual brush.
Both groups demonstrated statistically significant reduction in all RMNPI scores for weeks 1 and 12 (P≤ .040), except for the manual brush group in the gingival margin subregion and lingual gingival margin subregion and for the O-R brush group in the lingual gingival margin subregion all at week 1 (P≥ .322). At week 1 and week 12, the O-R brush produced statistically significantly greater reductions in all adjusted mean RMNPI scores than did the manual brush (P < .001), with the exception of the lingual surface gingival margin subregion at week 1. Reductions at week 12 ranged from 2.6 to 6.9 times greater for the O-R brush over the manual brush (Table 4).
There were no adverse events reported or observed in the study.
Discussion
Previous studies have demonstrated advantages of the novel Oral-B iO in Daily Clean mode with the Ultimate Clean brush head in reducing gingivitis and plaque and promoting transitions to gingival health when compared to manual18,20 and sonic19,22 toothbrushes. This study demonstrates consistent performance when the Oral-B iO brush is used in Sensitive mode with an extra gentle brush head. After 1 and 12 weeks of use, the O-R toothbrush reduced gingivitis scores and gingival bleeding sites by approximately three times more than the manual brush, and the odds ratio of transitioning from a "not healthy" to "healthy" gingival case status was four times greater for O-R users as early as week 1. Plaque reduction was consistently greater for the O-R brush than the manual brush from first use through 12 weeks.
The O-R brush also provided significantly higher gingivitis and plaque reductions than the manual brush in the plaque-prone lingual regions.26 At week 12, the difference in adjusted mean change from baseline number of bleeding sites was 3.2 times greater for the O-R brush group compared to the manual group for whole mouth, but 4.3 times greater for lingual surfaces. The disproportionate effectiveness in lingual areas demonstrated by the O-R brush with the Gentle Care brush head has also been shown in studies with the Oral-B Ultimate Clean brush head.18,20,22 Both brush heads are round providing optimized cleaning efficiency to lingual areas that are difficult to access. Subjects who chose to use the app with the O-R brush may have also achieved more even brushing across the dentition from the active position detection coaching feature.
Designed to provide thorough, gentle-feel cleaning, this brush head features a complex profiled trim. The overall concave shape precisely surrounds the tooth surface, and the convex trim patterns of the inner field and outer tufts are designed to adapt to a tooth's unique curvature (Figure 1). Thin bristles are softer than thick bristles,27 and the bristles of this O-R brush head are among the thinnest, softest, and most densely packed bristles in the Oral-B line. This brush head can be paired with the O-R brush's slower-speed, 2-minute Sensitive mode and smart pressure sensor17 for customized plaque removal designed to feel gentle but without compromising cleaning efficacy.
As with all toothbrushing studies, there is a logistical limitation in that subjects are not blind to their treatment group. However, the examiner was blind to treatment and was experienced in plaque and gingivitis assessments. Furthermore, use of the app with the O-R toothbrush was not required or evaluated, so it was not possible to assess the impact of behavior change on clinical outcomes. Future research could assess the impact of subjects' brushing experience with the extra gentle brush head used in the Sensitive mode on brushing behavior (eg, brushing time, appropriate pressure) via tracking usage of the app, as user experience may have contributed to better brushing habits in this trial. Such research could also evaluate efficacy and self-reported brushing experience among a population with established gingival pain.
Conclusion and Clinical Implications
The findings of this study demonstrate that patients seeking a gentle brushing experience may use the novel O-R brush with an extra gentle brush head and Sensitive mode without compromising on plaque reduction efficacy or attainment of gingival health benefits.
ACKNOWLEDGMENTS
The authors thank Marisa DeNoble Loeffler, MS, for medical writing assistance in the preparation of the manuscript. Medical writing assistance was funded by Procter & Gamble, Mason, Ohio.
Disclosure
Drs. Grender, Timm, and Adam are employees of The Procter & Gamble Company.
About the Authors
Julie Grender, PhD
Research Fellow Statistician, The Procter & Gamble Company, Mason, Ohio, USA
C. Ram Goyal, DDS
Principal Investigator, All Sum Research Center Ltd., Mississauga, Ontario, Canada
Jimmy Qaqish, BSc
Vice President, Clinical Operations, All Sum Research Center Ltd., Mississauga, Ontario, Canada
Hans Timm, PhD
Senior Scientist, Procter & Gamble Service GmbH,
Kronberg, Germany
Ralf Adam, PhD
Research Fellow, Procter & Gamble Service GmbH,
Kronberg, Germany
References
1. Li Y, Lee S, Hujoel P, et al. Prevalence and severity of gingivitis in American adults. Am J Dent. 2010;23(1):9-13.
2. Khan SA, Kong EF, Meiller TF, Jabra-Rizk MA. Periodontal diseases: bug induced, host promoted. PLoS Pathog. 2015;11(7):e1004952.
3. Ferreira MC, Dias-Pereira AC, Branco-de-Almeida LS, et al. Impact of periodontal disease on quality of life: a systematic review. J Periodontal Res. 2017;52(4):651-665.
4. Löe H, Theilade E, Jensen SB. Experimental gingivitis in man. J Periodontol. 1965;36:177-187.
5. Ower P. The role of self-administered plaque control in the management of periodontal diseases: I. A review of the evidence. Dent Update. 2003;30(2):60-68.
6. Ower P. The role of self-administered plaque control in the management of periodontal diseases: 2. Motivation, techniques and assessment. Dent Update. 2003;30(3):110-116.
7. Van der Weijden FA, Slot DE. Efficacy of homecare regimens for mechanical plaque removal in managing gingivitis a meta review. J Clin Periodontol. 2015;42(suppl 16):S77-S91.
8. Yaacob M, Worthington HV, Deacon SA, et al. Powered versus manual toothbrushing for oral health. Cochrane Database Syst Rev. 2014;2014(6):CD002281.
9. Pitchika V, Pink C, Völzke H, et al. Long-term impact of powered toothbrush on oral health: 11-year cohort study. J Clin Periodontol. 2019;46(7):713-722.
10. Deacon SA, Glenny AM, Deery C, et al. Different powered toothbrushes for plaque control and gingival health. Cochrane Database Syst Rev. 2010;2010(12):CD004971.
11. Grender J, Adam R, Zou Y. The effects of oscillating-rotating electric toothbrushes on plaque and gingival health: a meta-analysis. Am J Dent. 2020;33(1):3-11.
12. Clark-Perry D, Levin L. Systematic review and meta-analysis of randomized controlled studies comparing oscillating-rotating and other powered toothbrushes. J Am Dent Assoc. 2020;151(4):265-275.e6.
13. Thomassen TM, Van der Weijden FG, Slot DE. The efficacy of powered toothbrushes: a systematic review and network meta-analysis. Int J Dent Hyg. 2022;20(1):3-17.
14. Chapple IL, Mealey BL, Van Dyke TE, et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;89(suppl 1):S74-S84.
15. Elkerbout TA, Slot DE, Rosema NA, Van der Weijden GA. How effective is a powered toothbrush as compared to a manual toothbrush? A systematic review and meta-analysis of single brushing exercises. Int J Dent Hyg. 2020;18(1):17-26.
16. van der Sluijs E, Slot DE, Hennequin-Hoenderdos NL, et al. Dental plaque score reduction with an oscillating-rotating power toothbrush and a high-frequency sonic power toothbrush: a systematic review and meta-analysis of single-brushing exercises. Int J Dent Hyg. 2021;19(1):78-92.
17. Adam R. Introducing the Oral-B iO electric toothbrush: next generation oscillating-rotating technology. Int Dent J. 2020;70
(suppl 1):S1-S6.
18. Grender J, Goyal CR, Qaqish J, Adam R. An 8-week randomized controlled trial comparing the effect of a novel oscillating-rotating toothbrush versus a manual toothbrush on plaque and gingivitis. Int Dent J. 2020;70(suppl 1):S7-S15.
19. Adam R, Goyal CR, Qaqish J, Grender J. Evaluation of an oscillating-rotating toothbrush with micro-vibrations versus a sonic toothbrush for the reduction of plaque and gingivitis: results from a randomized controlled trial. Int Dent J. 2020;70(suppl 1):S16-S21.
20. Adam R, Erb J, Grender J. Randomized controlled trial assessing plaque removal of an oscillating-rotating electric toothbrush with micro-vibrations. Int Dent J. 2020;70(suppl 1):S22-S27.
21. Goldschmidtboeing F, Pelz U, Claire-Zimmet K, et al. Bristle motion, forces, and related vertical translation for a novel electric toothbrush design. J Mech Eng. 2020;66(9):505-512.
22. Goyal CR, Adam R, Timm H, et al. A 6-month randomized controlled trial evaluating a novel smart-connected oscillating-rotating toothbrush versus a smart-connected sonic toothbrush for the reduction of plaque and gingivitis. Am J Dent. 2021;34(1):54-60.
23. Lobene RR, Weatherford T, Ross NM, et al. A modified gingival index for use in clinical trials. Clin Prev Dent. 1986;8(1):3-6.
24. Rustogi KN, Curtis JP, Volpe AR, et al. Refinement of the Modified Navy Plaque Index to increase plaque scoring efficiency in gumline and interproximal tooth areas. J Clin Dent. 1992;3(suppl C):C9-C12.
25. Saxton CA, van der Ouderaa FJ. The effect of a dentifrice containing zinc citrate and Triclosan on developing gingivitis. J Periodontal Res. 1989;24(1):75-80.
26. White DJ. Dental calculus: recent insights into occurrence, formation, prevention, removal and oral health effects of supragingival and subgingival deposits. Eur J Oral Sci. 1997;105(5 Pt 2):508-522.
27. Ng C, Tsoi JKH, Lo ECM, Matinlinna AJP. Safety and design aspects of powered toothbrush - a narrative review. Dent J (Basel). 2020;8(1):15.
Figures and Images
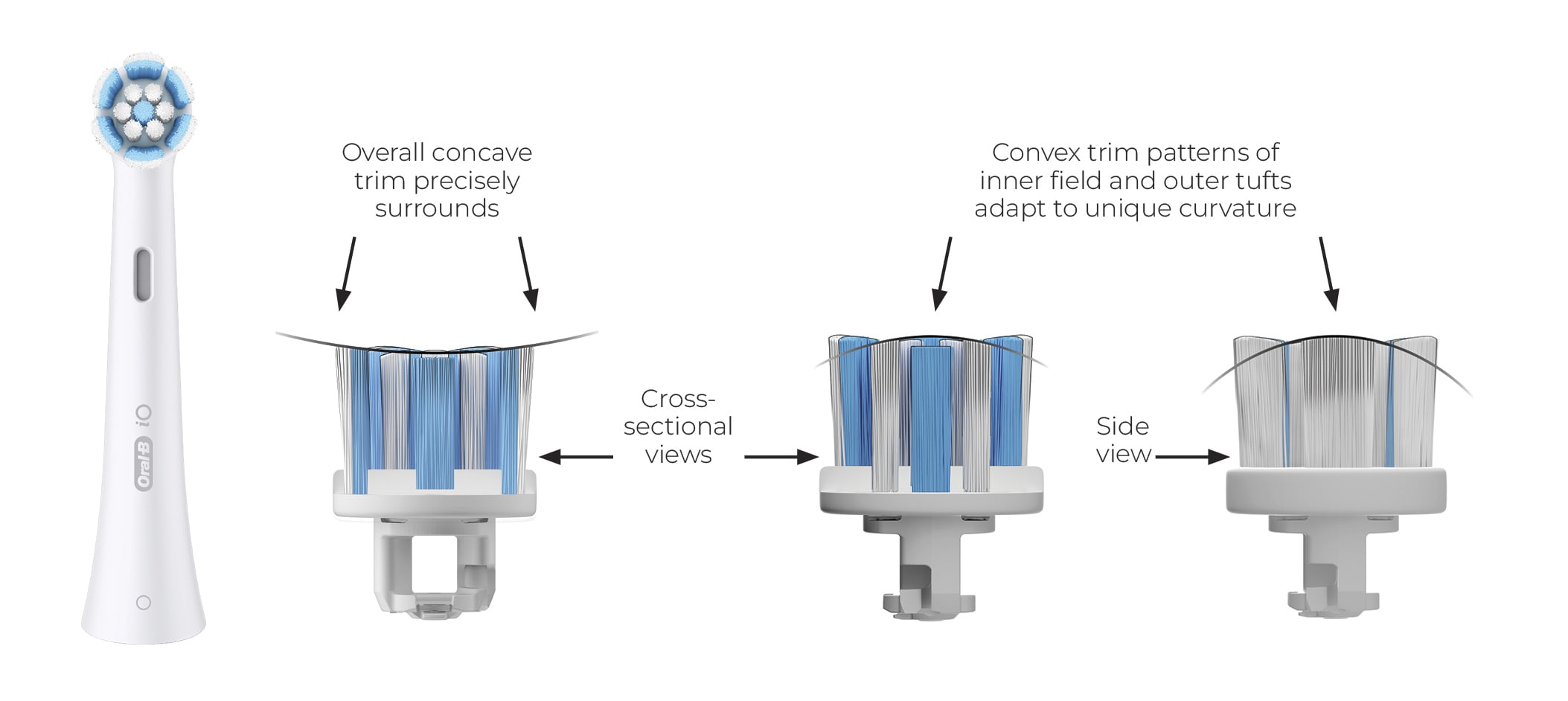
Figure 1
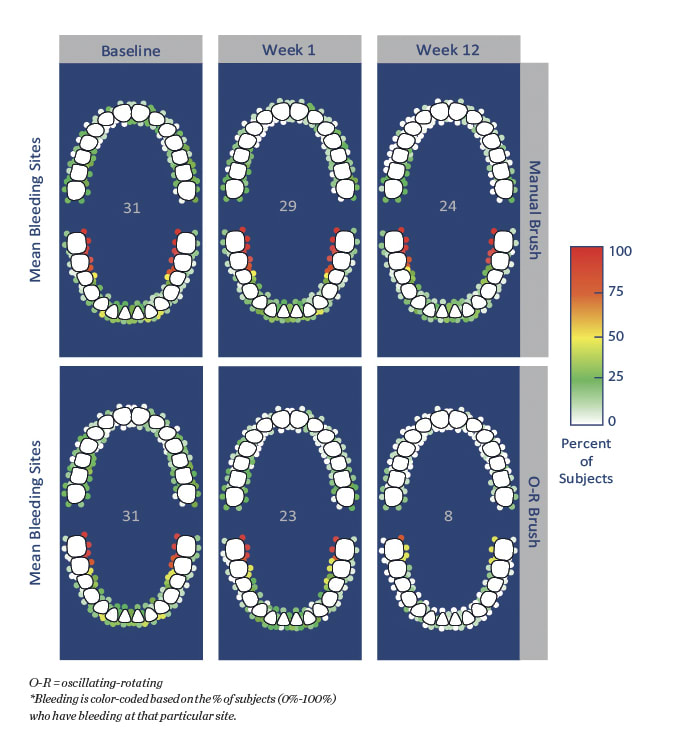
Figure 2

Table 1
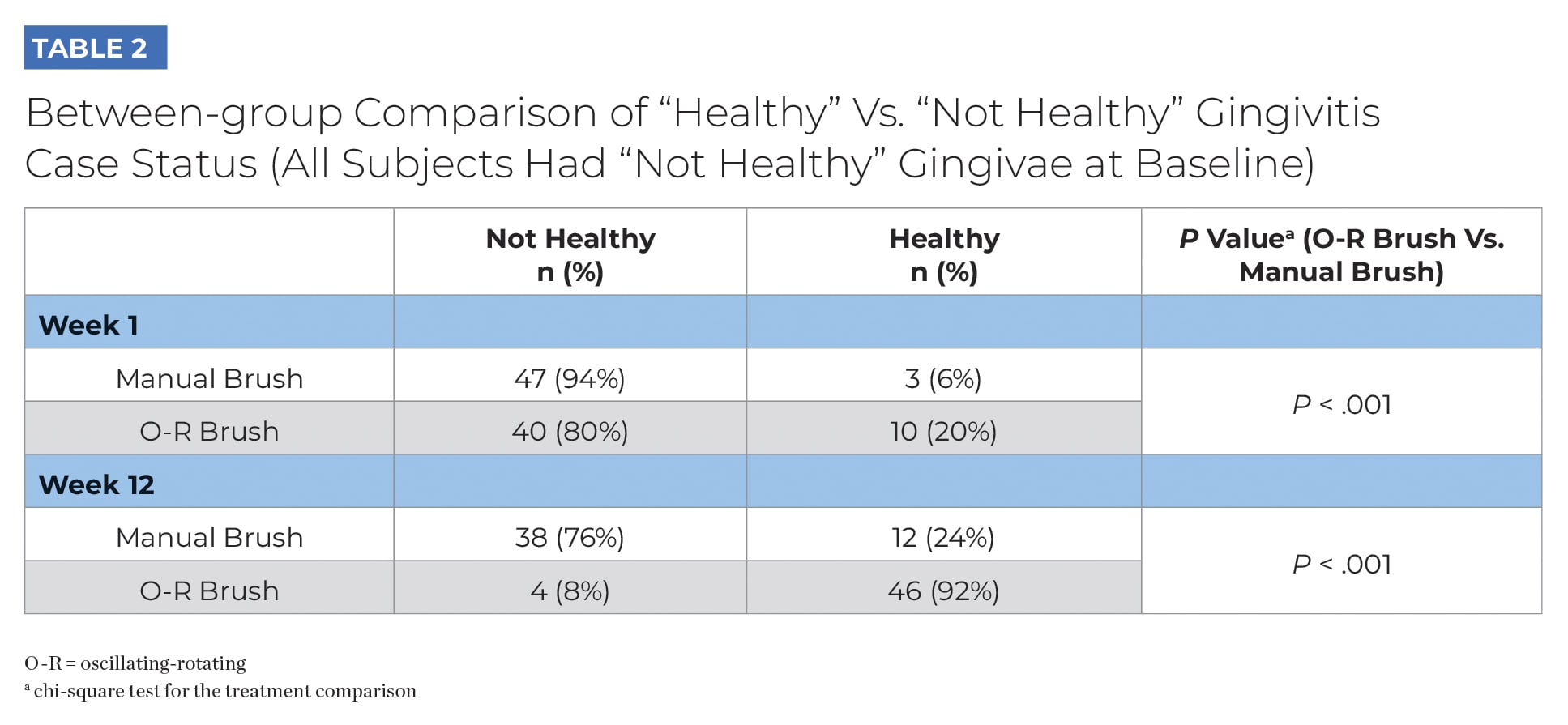
Table 2
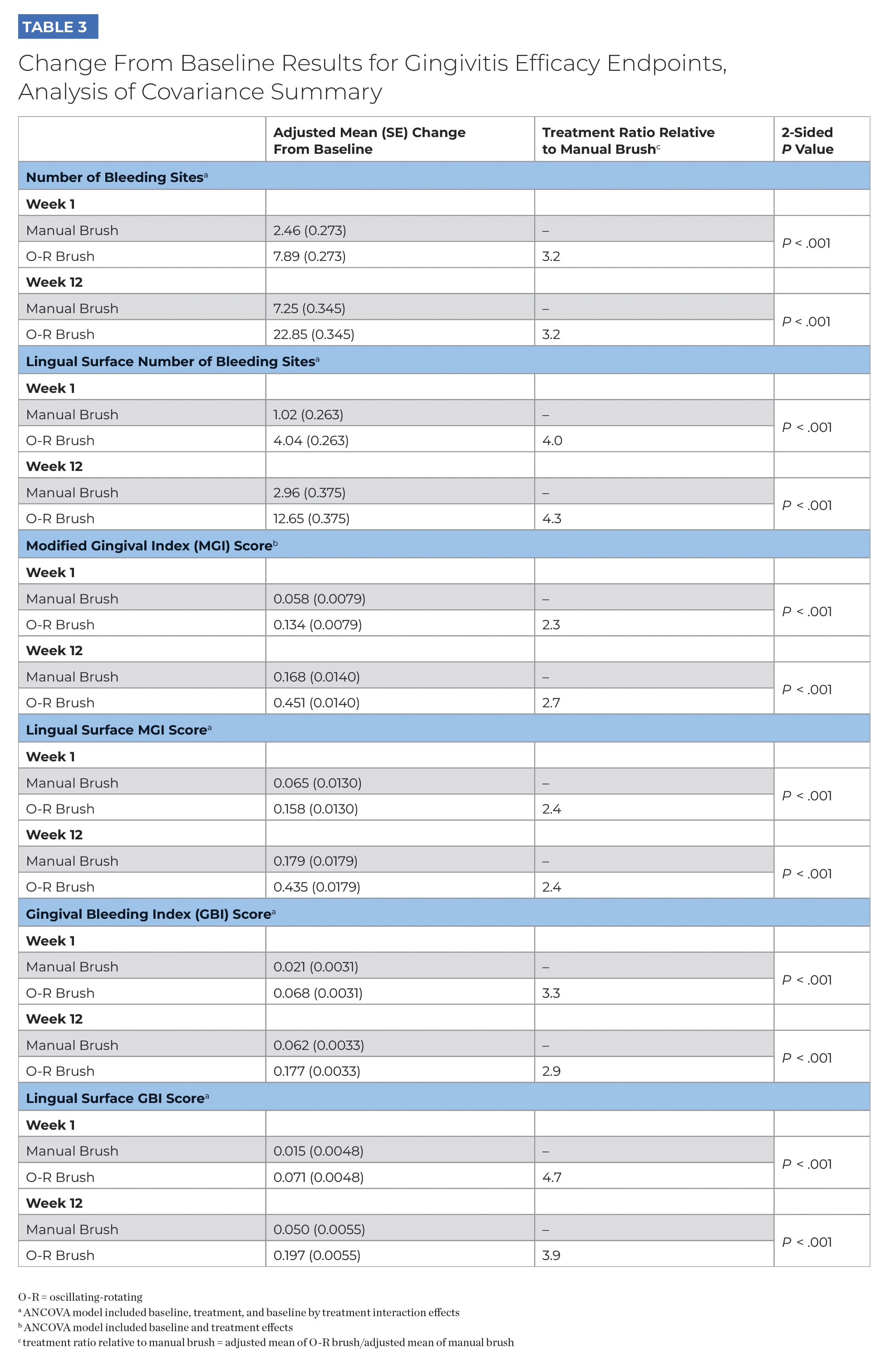
Table 3
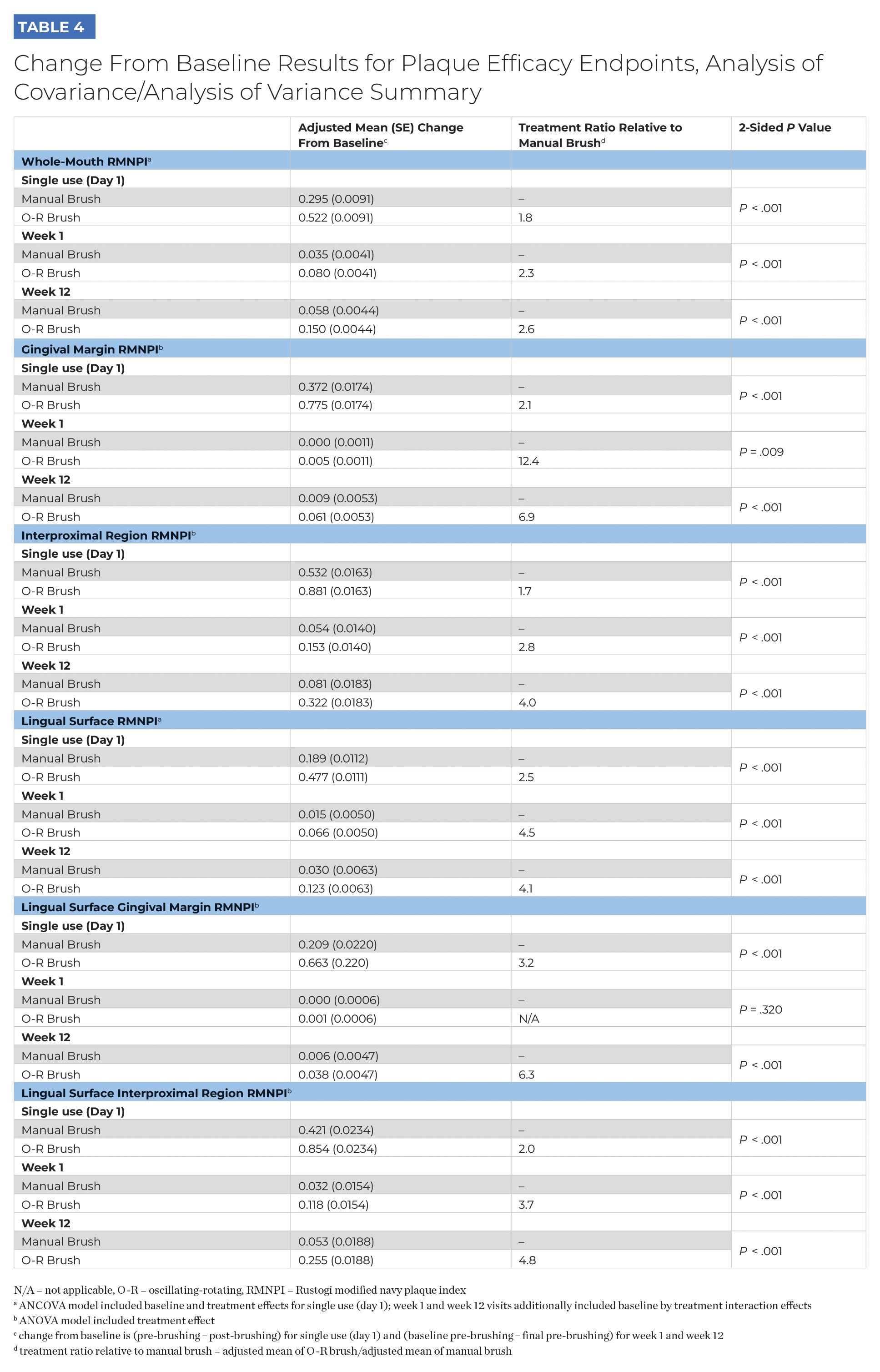
Table 4
