Abstract:
Mini dental implants are becoming increasingly popular in dental care today. Because of their smaller size they are often used in cases of limited bone anatomy. Mini dental implants have diameters ranging from 1.8 mm to 3 mm and are suitable for long-term use. This article describes a retrospective analysis of 5640 mini dental implants placed into 1260 patients over a 12-year period. The mean length of follow-up was 3.5 years. The implants placed supported removable (2319) and fixed prostheses (3321), with placement in the maxilla (3134) and mandible (2506). The overall implant survival was 92.1%. Failures of implants (445) were attributed to mobility of the implant; the mean time to failure for these implants was 14.4 months. The small size of these implants has led to the development of techniques that enable placement and use in a short amount of time for both the doctor and patient. The high rates of success show that mini dental implants are suitable for use in supporting fixed and removable prosthetics.
Implant dentistry has changed significantly in the past several decades. Since the early investigations of Brånemark that led to the dental application of osseointegration,1 the field of dental implantology has evolved rapidly. Although technology has improved greatly over the past several years, and some conventional implant systems allow for early loading, most conventional endosseous fixtures require up to 4 to 6 months or longer before prosthetic restoration can be completed.2 In addition, often times these larger-diameter implants require sinus lift procedures and bone augmentation. Using mini dental implants that enable immediate denture stabilization, or single and multiple-tooth replacement in as little as one visit,3 is clearly desirable to patients. The relatively lower cost of mini dental implants allows for a larger patient-selection base. Christensen described these implants as simple, predictable, minimally invasive, and relatively inexpensive.4 Additionally, the osseointegration period required for mini dental implants can be significantly shorter than that for conventional implants because of a less aggressive insertion procedure (ie, minimized disruption of the periosteum).
Mini dental implants were initially designed for the temporary stabilization of a prosthesis during the healing period of conventional implants.5 Recently, they have become popular in use for orthodontic anchorage,6-8 periodontal therapy,9 fixed prosthetics, and complete denture stabilization.10
Because mini implant insertion requires minimal disruption of the periosteum, there is reduced damage to the insertion area.2 Mini dental implants and their function in immediate loading for denture stabilization and fixed restorations have become increasingly prevalent in the literature. Ahn and colleagues reported 26 of 27 mini dental implants were stable in the mandible at 21 weeks of follow-up.11 A previous study by the primary author of 2514 mini dental implants placed in the mandible and maxilla reported an average overall implant survival rate of 94.1%.3 In a multi-clinic evaluation of mini dental implant use in denture stabilization, Bulard and Vance reported similar results with approximately 90% success rates.2 This article describes a retrospective analysis of 5640 mini dental implants used in various treatment modalities in 1260 patients, showing an overall implant survival rate of 92.1%.
Surgical Procedure
A panoramic roentgenogram or cone beam computed tomography scan was completed to assess bone parameters and plan implant placement sites. Consider the example of the stabilization of a maxillary and mandibular denture (Figure 1). The placement sites were marked on the radiograph between the canine and first bicuspid anterior to the mental foramen as well as in the region of lateral incisors anteriorly (Figure 2). Next, depending on the size and type of prosthesis, the quantity of mini implants to use was determined. The primary author recommends the placement of four mini implants for the stabilization of a full mandibular denture. While four mini implants may also be sufficient for a maxillary denture stabilization procedure, six are recommended if a palateless denture is being considered. For single tooth replacement one mini implant is used for anterior and bicuspid teeth, while for molars, often two mini implants are used.12,13 In this context, occlusal and masticatory forces are distributed over an augmented implant interface; the relative strain on any implant is reduced.13 Furthermore, the bridgework in these cases acts as a splint, anchoring adjacent implants and reducing micro-movement.13 Similarly, adjacent missing teeth replaced using mini dental implants should be splinted together.
The next step was to determine the appropriate mini dental implant size. The longest mini dental implant possible for the available bone should always be used.14 Mini implants do not utilize deep bone osteotomies like conventional implant systems require. The minimally invasive nature of using a small 1.2-mm pilot drill to a depth of only a portion of the mini implant length avoids the possibility of osteonecrosis from over-drilling bone. In this study or otherwise, the primary author has not encountered any cases of osteonecrosis with mini implants, even in patients who are immunocompromised or taking multiple medications. For a detailed study on implant size selection, see the noted references.15
Next, the surgical stent was placed in the patient’s mouth and marks were placed through the stent openings using a marking stick (Figure 3 and Figure 4). These marks were used to confirm planned implant placement positions. Infiltration anesthesia was then used between the periosteum and bone. Local anesthetic was injected on the mark, lingual to the mark, and buccal to the mark, at each location. Though a local anesthesia block of the inferior alveolar nerve is used in many dental procedures, it is not recommended for mini dental implant placement.16 This is because using infiltration affords the patient continued sensation of the inferior alveolar nerve, which allows the patient to offer feedback during the procedure, thus reducing the risk of nerve damage.
The pilot hole for the mini implants was then made using a 1.2-mm pilot drill (approximately half the diameter of the mini implants). Using sterile surgical techniques17 the dentist drilled to the appropriate depth based on bone density evaluation and implant type selected. For very dense bone, a pilot hole was drilled to be 80% of the length of the implant. For moderately dense bone, the pilot hole depth was 60% of the length of the implant. For low-density bone (maxillary bone or soft mandibular spongy bone) the pilot hole was created at 50% the length of the mini implant. Because of the flapless surgical technique most often utilized with mini implants, a surgical stent (Figure 5) designed from preoperative dental models, x-rays, and/or cone beam CT scans provides for proper angulation in the bone. A pilot drill guide (Figure 6) was used to position the pilot hole in the center of the surgical stent sleeve and maintain correct trajectory of the drill.18,19 The pilot drill was used to puncture the tissue down to the bone, and after locating the bone surface the pilot hole was made with a tapping motion.
The implant was first removed from its package using either the finger driver or a contra angle adapter. This prevented the sterile surface of the implant from being contaminated. The implant was then inserted into the pilot opening through the surgical stent and gingiva, and into the bone. The implant was slowly rotated clockwise (with a drill or hand instrumentation) using downward pressure until firm, bony resistance was detected. The implant was inserted until all threads were subgingival and the top of the polished collar was flush with the top of the gingiva. At this point the clinician knows that the implant is seated to the proper depth of placement (Figure 7). If extremely dense bone was present, as is often the case in the anterior mandible, a ratchet wrench was used for the final rotations of implant insertion. The ratchet wrenching was done using very slow incremental turns, which allowed full insertion of the implant without implant fracture or stripping of bone. If very heavy resistance was noticed, the implant was removed by rotation in the reverse direction and the pilot hole was made deeper, or a shorter implant was used. Through the entire rotation procedure, pressure was constantly applied on the head of the ratchet in the direction of desired insertion.
The mini dental implants used in this study were inserted such that the square neck portion of the implant was supragingival. O-ring housing abutments were then placed on the O-balls of the mini implants (Figure 8). With a pear-shaped laboratory bur, holes were placed in the patient’s denture at the previously marked locations. The denture was tried in the patient’s mouth for full seating. The holes in the denture were then filled with a housing resin or cold-cure acrylic. Before these materials set, the denture was placed on the O-ring housings and seated firmly. The patient was instructed to bite down for 3 to 5 minutes. The denture was then removed and the firmness of the housings was assessed. If housings were loose, the appropriate acrylic was applied. The denture with housings was then smoothed and adjusted to avoid patient discomfort and sore spot development (Figure 9). A postoperative radiograph can be seen in Figure 10.
Postoperative instructions were given to the patient, and an appointment was scheduled for 24 hours after placement. Patients were told to wear their dentures continuously for the first 24 hours to allow the tissue surrounding the implants to heal without advancing up around the neck and O-balls of the implants. It is important that any dentist considering using mini dental implants be adequately educated in the surgical aspects of implant placement.
The primary author developed the Fabricated Implant Restoration and Surgical Technique (F.I.R.S.T.®) (Patent: USPTO #7,108,511 B; September 2006), which enables the placement of mini dental implants and permanent crowns to be cemented in a single visit (Figure 11 through Figure 15).
Materials and Methods
From January 10, 2000, to February 8, 2012, 5640 implants were placed in 1260 patients. All patients received treatment in a private office setting. Most patients were selected for implant placement based on subjective complaints such as concern about denture reliability in social settings, difficulty wearing an upper or lower denture, cosmetic concerns from missing teeth, and the desire to feel more confident. Objective reasons for mini dental implant placement included denture stabilization on a narrow alveolar ridge, single missing teeth, and partial or complete edentulism. There were minimal exclusion criteria; severely atrophic or poor quality bone was considered.
Twelve years and 1 month after the first mini dental implant in this study was placed, a review of patient charts was performed to assess implant survival. Success criteria included some of those described by Buser et al20: 1) absence of continual subjective complaints such as pain or foreign body sensation; 2) absence of mobility; 3) absence of recurrent peri-implant infection with suppuration; and 4) absence of continuous radiolucency around the implant.
When mobility of a fixed prosthetic was present, it was removed and implants were individually assessed. If a fixed prosthesis was stable, and the above success criteria observed in this study were met, it was assumed that all underlying implants were stable.
Patient variables were obtained from the dental record. These included age, sex, date of birth, implant placement date, type of prosthesis (upper or lower partial denture, upper or lower full denture, fixed upper or lower prosthesis, or single tooth restoration), implant size (diameter and length), anatomical location (anterior or posterior, maxillary or mandibular), smoking status, and date of previous implant failure (if applicable). The date of most recent follow-up was also recorded. Overall implant survival was then determined along with survival rates based on some of the above listed patient variables.
Results
The mean duration of follow-up was 3.5 years. Of the 5640 implants placed, 445 failures were recorded, giving an overall survival rate of 92.1%. The mean time to failure for this series was 14.4 months.
The distribution of implants used for each treatment modality is shown in Table 1. There were 2506 implants placed into the mandible and 3134 placed into the maxilla. Analysis of implant survival in the mandible and maxilla revealed similar survival rates of 93.1% and 91.3%, respectively. Survival based on each modality revealed that implants supporting partial lower dentures fared the best, with a survival rate of 95.6%, while those supporting full upper dentures fared the worst, with 85.2% survival (Figure 16).
Implants supporting fixed prostheses were considerably more successful than those supporting removable prostheses, having success rates of 94.7% and 88.4%, respectively. Further analysis of location of placement revealed a lower mini implant success rate in the maxilla (90.3% anterior; 92.5% posterior) relative to the mandible (92.3% anterior; 94.1% posterior). The reduced implant success rate in the maxilla was likely due to its poorer bone quality relative to the mandible. Though there exists greater occlusion in the posterior regions of the mouth, higher implant success rates in those areas may be attributed to the use of multiple implants to support a prosthesis, mimicking the natural root anatomy. Often, two implants were used to replace single molars and multiple implants were used for posterior restorations involving more than one tooth.
Gender also played a role in the survival of implants. Of the 3378 implants placed in females, the overall success was 93.0%, while the success rate of the 2262 implants placed in males was only 90.8%.
Implants were placed in patients aged 13 years old to 95 years old. The distribution of implants by patient’s age is shown in Figure 17. Patients 21 to 30 years of age had the highest rate of success at 95.8%.
There were 445 implant failures observed. Implants considered as failed presented as being mobile or fractured. Of those implants that failed, the majority did so in the first 6 months following implantation. Implants not failing in this time following insertion likely attained osseointegration. This correlates with Brånemark’s classical definition of osseointegration of 3 to 6 months in the mandible and 6 to 9 months in the maxilla.21
Conclusion
With the growing demand from patients for fewer office visits, lower cost procedures with immediate results, and shorter recovery time, dental rehabilitation techniques have been developed for minimally invasive, single-stage implant placement. The mini dental implants used in these procedures have been demonstrated to have high success rates. Over a 12-year period, 5640 mini dental implants were placed with an overall survival of 92.1%. With the proper training,22 consideration for prosthetic subtype, implant location, size, and patient variables, mini dental implants can provide exceptional outcomes. These results are rewarding for the dentist, minimally invasive and affordable to the patient, and have long-term success for both fixed and removable prosthetics.
Disclosure
Dr. Shatkin is the owner of Shatkin F.I.R.S.T.®
About the Authors
Todd Ellis Shatkin, DDS
Private Practice
Buffalo, New York
Christopher Anthony Petrotto
Pre-dentistry student at Canisius College
Buffalo, New York
References
1. Taylor TD, Agar JR. Twenty years of progress in implant prosthodontics. J Prosthet Dent. 2002;88(1):89-95.
2. Bulard RA, Vance JB. Multi-clinic evaluation using mini-dental implants for long-term denture stabilization: a preliminary biometric evaluation. Compend Contin Educ Dent. 2005;26(12):892-897.
3. Shatkin TE, Shatkin S, Oppenheimer BD, Oppenheimer AJ. Mini dental implants for long-term fixed and removable prosthetics: a retrospective analysis of 2514 implants placed over a five-year period. Compend Contin Educ Dent. 2007:28(2):92-99.
4. Christensen GJ. The increased use of small-diameter implants. J Am Dent Assoc. 2009;140(6):709-712.
5. Sendax VI. Mini-implants as adjuncts for transitional prostheses. Dent Implantol Update. 1996;7(2):12-15.
6. Baumgaertel S, Razavi MR, Hans MG. Mini-implant anchorage for the orthodontic practitioner. Am J Orthod Dentofacial Orthop. 2008;133(4):621-627.
7. Chen Y, Kyung HM, Zhao WT, Yu WJ. Critical factors for the success of orthodontic mini-implants: a systematic review. Am J Orthod Dentofacial Orthop. 2009;135(3):284-291.
8. Ren Y. Mini-implants for direct or indirect orthodontic anchorage. Evid Based Dent. 2009;10(4):113.
9. Nagata M, Nagaoka S. Preservation of the natural teeth and arch integrity by the use of transitional mini-implants. J Periodontol. 2000;71(12):1910.
10. Hoos JC. An overview of mini-implants and their role in complete denture treatment. Dent Econ. 2011:101(4):2-16.
11. Ahn MR, An KN, Cho JH, Sohn DS. Immediate loading with mini dental implants in the fully edentulous mandible. Implant Dent. 2004;13(4):367-372.
12. Henry PJ. Tooth loss and implant replacement. Aust Dent J. 2000;45(3):150-172.
13. Weiss CM, Weiss A. Principles and Practice of Implant Dentistry. St Louis, Mo: Mosby Inc.; 2001.
14. Olate S, Lyrio MC, de Moraes M. Influence of diameter and length of implant on early dental implant failure. J Oral Maxillofac Surg. 2010;68(2):414-419.
15. Callan DP. Current concepts in selecting dental implant diameter size. Dent Implantol Update. 2004;15(3):17-23.
16. Heller AA, Shankland WE II. Alternative to the inferior alveolar nerve block anesthesia when placing mandibular dental implants posterior to the mental foramen. J Oral Implantol. 2001;27(3):127-133.
17. Friberg B. Sterile operating conditions for the placement of intraoral implants. J Oral Maxillofac Surg. 1996;54(11):1334-1336.
18. Choi M, Romberg E, Driscoll CF. Effects of varied dimensions of surgical guides on implant angulations. J Prosthet Dent. 2004;92(5):463-469.
19. Lewis S, Avera S, Engleman M, Beumer J III. The restoration of improperly inclined osseointegrated implants. Int J Oral Maxillofac Implants. 1989:4(2):147-152.
20. Buser D, Meriscke-Stern R, Bernard JP, et al. Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multi-center study with 2359 implants. Clin Oral Implants Res. 1997;8(3):161-172.
21. Brånemark PI. The Osseointegration Book: from Calvarium to Calcaneus. Berlin, Germany: Quintessence Publishing; 2005:215-225.
22. Christensen GJ. The “mini”-implant has arrived. J Am Dent Assoc. 2006;137(3):387-390.
Click here to download a PDF of Shatkin F.I.R.S.T.® Crown and Bridge Procedural Guide
Click Here to download a PDF of Shatkin F.I.R.S.T.® Denture Stabilization Procedural Guide
Figures and Images

Table 1

Figure 1
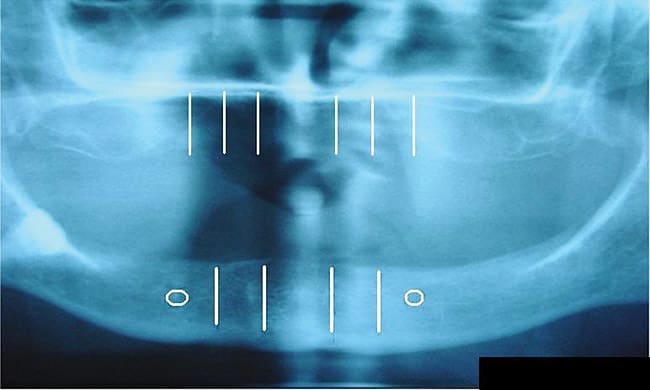
Figure 2

Figure 3

Figure 4

Figure 5
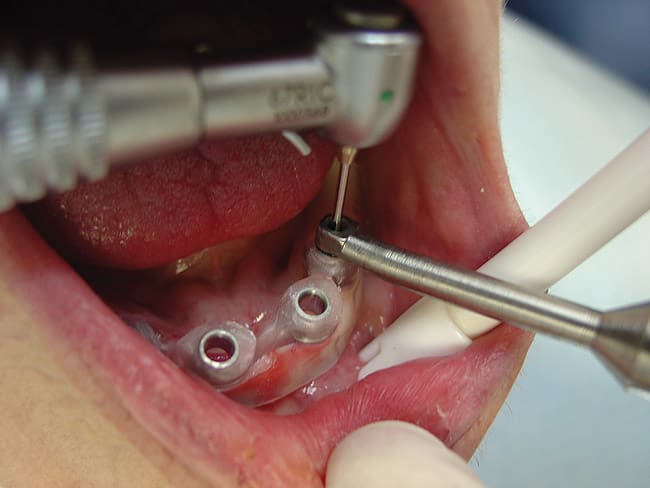
Figure 6

Figure 7

Figure 8

Figure 9

Figure 10

Figure 11

Figure 12

Figure 13

Figure 14

Figure 15
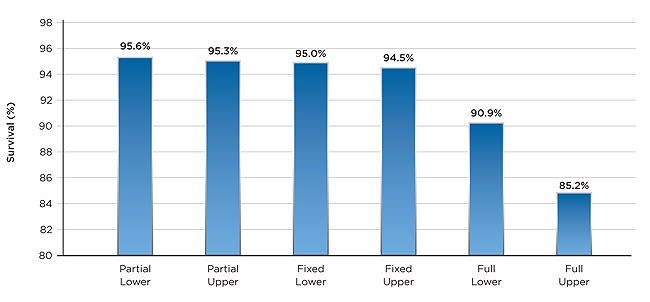
Figure 16

Figure 17
